

Management of congenital nephrotic syndrome: consensus recommendations of the ERKNet-ESPN Working Group
- PMID: 33514942
- PMCID: PMC8128706
- DOI: 10.1038/s41581-020-00384-1
Management of congenital nephrotic syndrome: consensus recommendations of the ERKNet-ESPN Working Group
Erratum in
-
Publisher Correction: Management of congenital nephrotic syndrome: consensus recommendations of the ERKNet-ESPN Working Group.Nat Rev Nephrol. 2021 Jun;17(6):434. doi: 10.1038/s41581-021-00431-5. Nat Rev Nephrol. 2021. PMID: 33941901 Free PMC article. No abstract available.
Abstract
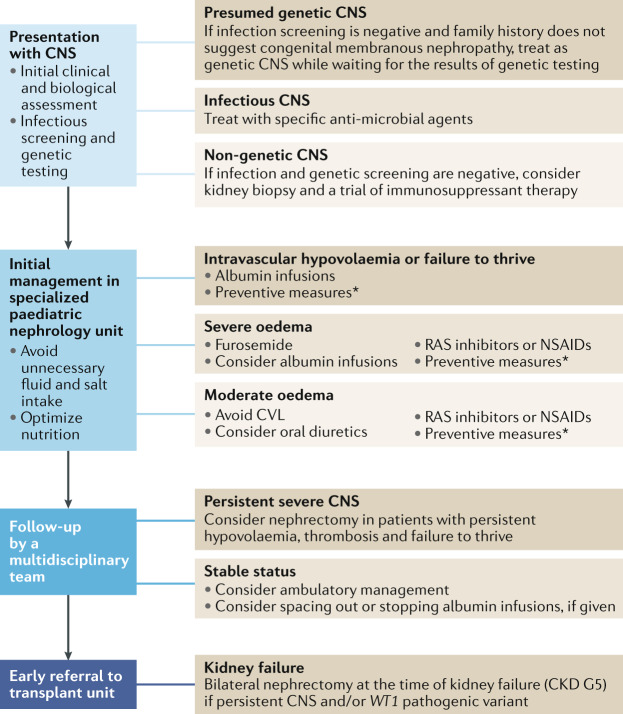
Congenital nephrotic syndrome (CNS) is a heterogeneous group of disorders characterized by nephrotic-range proteinuria, hypoalbuminaemia and oedema, which manifest in utero or during the first 3 months of life. The main cause of CNS is genetic defects in podocytes; however, it can also be caused, in rare cases, by congenital infections or maternal allo-immune disease. Management of CNS is very challenging because patients are prone to severe complications, such as haemodynamic compromise, infections, thromboses, impaired growth and kidney failure. In this consensus statement, experts from the European Reference Network for Kidney Diseases (ERKNet) and the European Society for Paediatric Nephrology (ESPN) summarize the current evidence and present recommendations for the management of CNS, including the use of renin-angiotensin system inhibitors, diuretics, anticoagulation and infection prophylaxis. Therapeutic management should be adapted to the clinical severity of the condition with the aim of maintaining intravascular euvolaemia and adequate nutrition, while preventing complications and preserving central and peripheral vessels. We do not recommend performing routine early nephrectomies but suggest that they are considered in patients with severe complications despite optimal conservative treatment, and before transplantation in patients with persisting nephrotic syndrome and/or a WT1-dominant pathogenic variant.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Holmberg C, Antikainen M, Ronnholm K, Ala Houhala M, Jalanko H. Management of congenital nephrotic syndrome of the Finnish type. Pediatr. Nephrol. 1995;9:87–93. - PubMed
-
- Buscher AK, Weber S. Educational paper: the podocytopathies. Eur. J. Pediatr. 2012;171:1151–1160. - PubMed
-
- Kestila M, et al. Positionally cloned gene for a novel glomerular protein — nephrin — is mutated in congenital nephrotic syndrome. Mol. Cell. 1998;1:575–582. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
