

Oral insulin immunotherapy in children at risk for type 1 diabetes in a randomised controlled trial
- PMID: 33515070
- PMCID: PMC8012335
- DOI: 10.1007/s00125-020-05376-1
Oral insulin immunotherapy in children at risk for type 1 diabetes in a randomised controlled trial
Abstract
Aims/hypothesis: Oral administration of antigen can induce immunological tolerance. Insulin is a key autoantigen in childhood type 1 diabetes. Here, oral insulin was given as antigen-specific immunotherapy before the onset of autoimmunity in children from age 6 months to assess its safety and immune response actions on immunity and the gut microbiome.
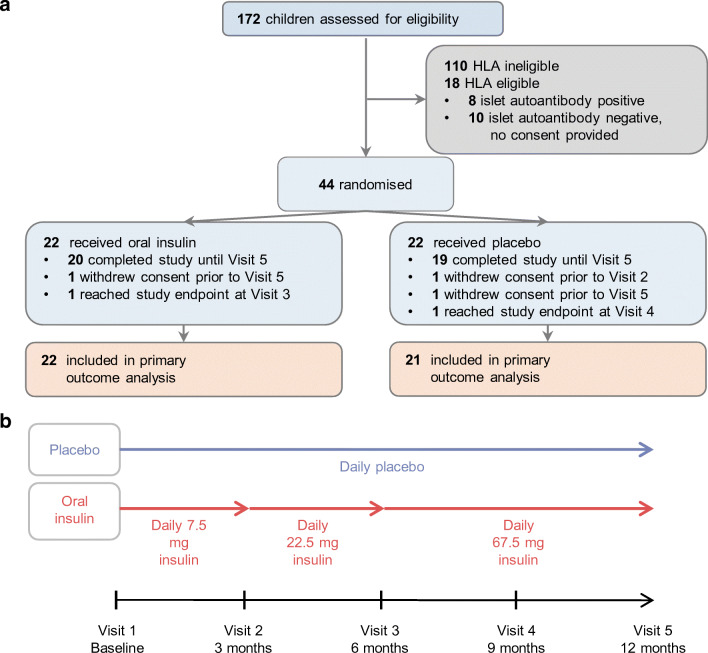
Methods: A phase I/II randomised controlled trial was performed in a single clinical study centre in Germany. Participants were 44 islet autoantibody-negative children aged 6 months to 2.99 years who had a first-degree relative with type 1 diabetes and a susceptible HLA DR4-DQ8-containing genotype. Children were randomised 1:1 to daily oral insulin (7.5 mg with dose escalation to 67.5 mg) or placebo for 12 months using a web-based computer system. The primary outcome was immune efficacy pre-specified as induction of antibody or T cell responses to insulin and measured in a central treatment-blinded laboratory.
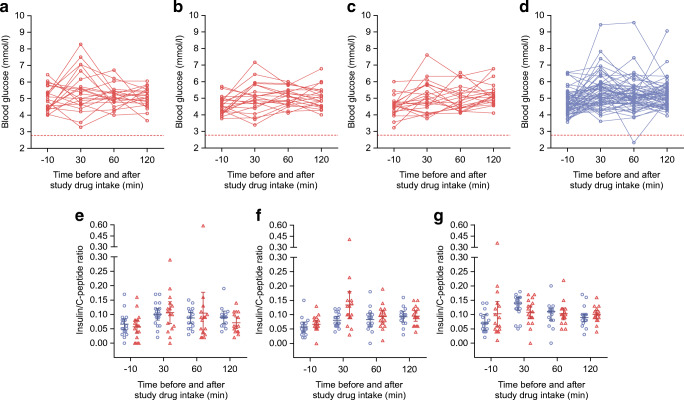
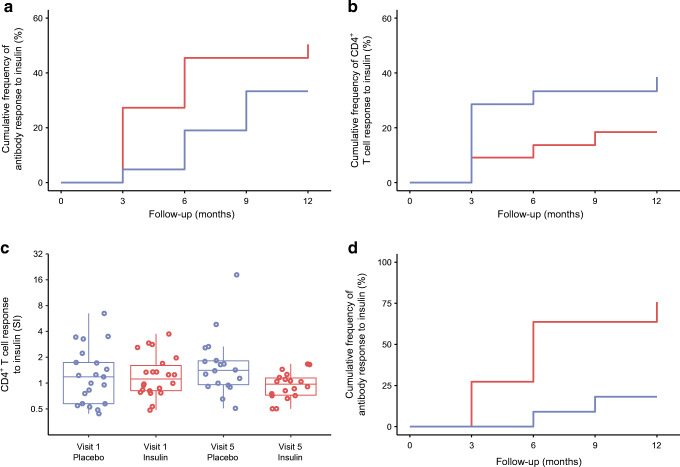
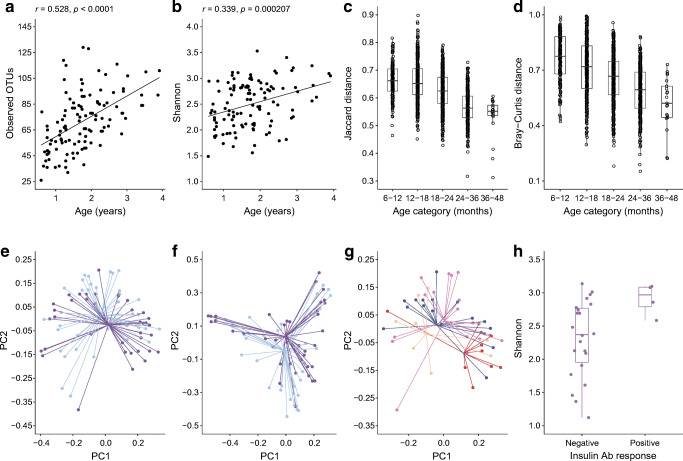
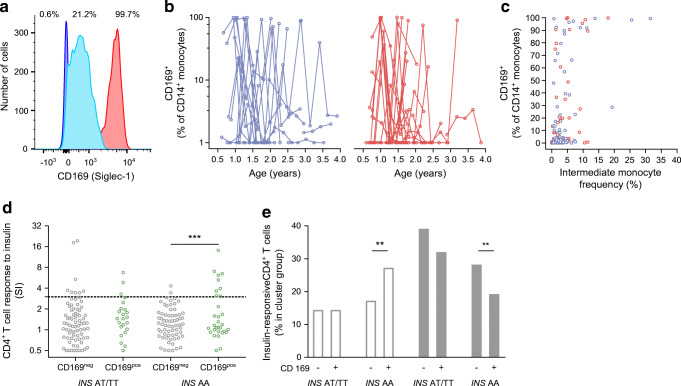
Results: Randomisation was performed in 44 children. One child in the placebo group was withdrawn after the first study visit and data from 22 insulin-treated and 21 placebo-treated children were analysed. Oral insulin was well tolerated with no changes in metabolic variables. Immune responses to insulin were observed in children who received both insulin (54.5%) and placebo (66.7%), and the trial did not demonstrate an effect on its primary outcome (p = 0.54). In exploratory analyses, there was preliminary evidence that the immune response and gut microbiome were modified by the INS genotype Among children with the type 1 diabetes-susceptible INS genotype (n = 22), antibody responses to insulin were more frequent in insulin-treated (72.7%) as compared with placebo-treated children (18.2%; p = 0.03). T cell responses to insulin were modified by treatment-independent inflammatory episodes.
Conclusions/interpretation: The study demonstrated that oral insulin immunotherapy in young genetically at-risk children was safe, but was not associated with an immune response as predefined in the trial primary outcome. Exploratory analyses suggested that antibody responses to oral insulin may occur in children with a susceptible INS genotype, and that inflammatory episodes may promote the activation of insulin-responsive T cells.
Trial registration: Clinicaltrials.gov NCT02547519 FUNDING: The main funding source was the German Center for Diabetes Research (DZD e.V.).
Keywords: Autoimmunity; Insulin; Oral immunotherapy; Primary prevention; Type 1 diabetes.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
