

The role of serum C-reactive protein in the diagnosis of periprosthetic shoulder infection
- PMID: 33515325
- PMCID: PMC9296386
- DOI: 10.1007/s00402-021-03779-2
The role of serum C-reactive protein in the diagnosis of periprosthetic shoulder infection
Abstract
Introduction: There is a paucity of literature regarding serum C-reactive protein (CRP) in the evaluation of a shoulder periprosthetic joint infection (PJI). The purpose of the current study was to establish cutoff values for diagnosing shoulder PJI and evaluate the influence of the type of infecting microorganism and the classification subgroups according to last proposed International Consensus Meeting (ICM) criteria on the CRP level.
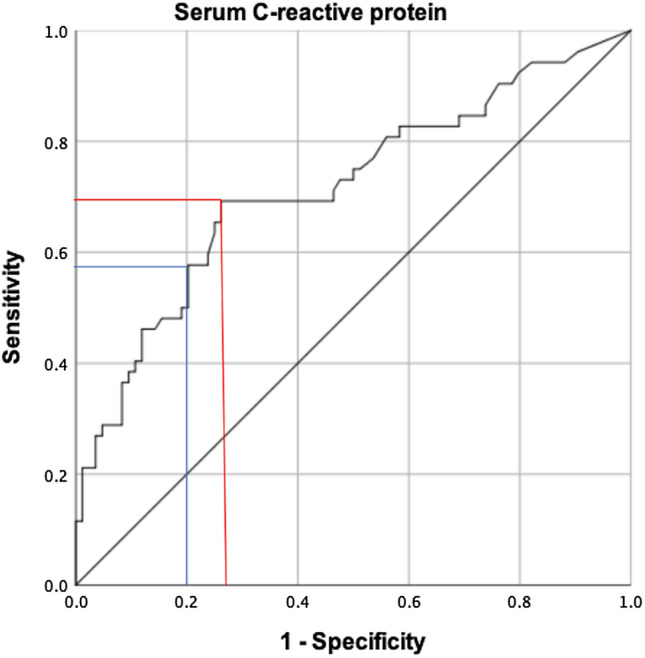
Materials and methods: A retrospective analysis of all 136 patients, who underwent septic or aseptic revision shoulder arthroplasty in our institution between January 2010 and December 2019, was performed. Shoulder PJI was defined according to the last proposed definition criteria of the ICM. Serum CRP levels were compared between infected and non-infected cases, between infection subgroups, as well as between different species of infecting microorganisms. A receiver-operating characteristic (ROC) analysis was performed to display sensitivity and specificity of serum CRP level for shoulder PJI.
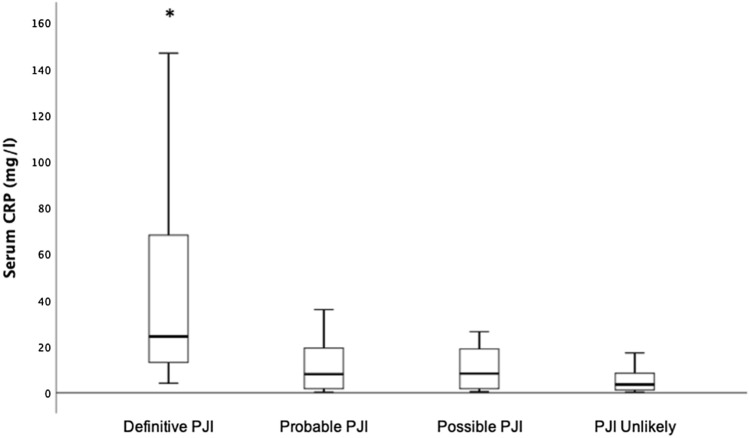
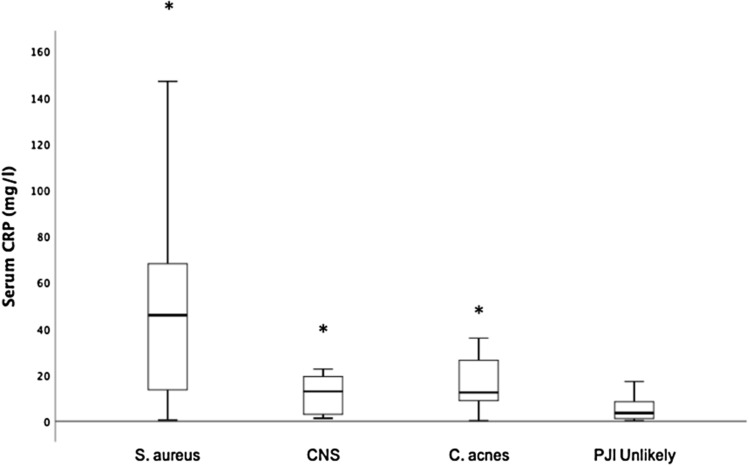
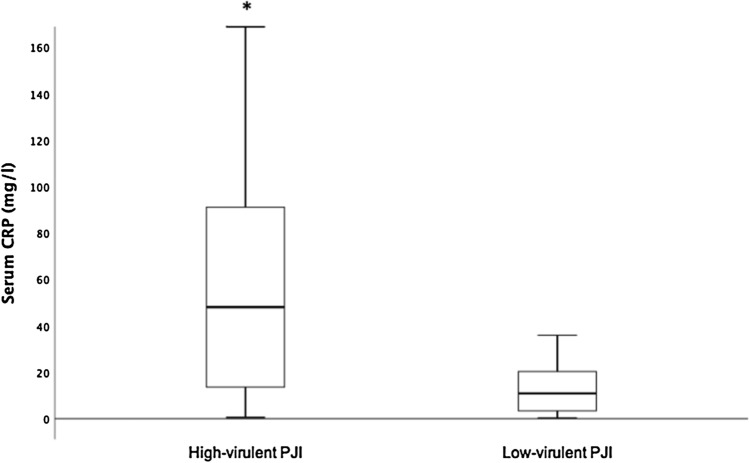
Results: A total of 52 patients (38%) were classified as infected, 18 meeting the criteria for definitive infection, 26 for probable infection and 8 for possible infection. According to the ROC curve, an optimized serum CRP threshold of 7.2 mg/l had a sensitivity of 69% and specificity of 74% (area under curve = 0.72). Patients with definitive infection group demonstrated significantly higher median serum CRP levels (24.3 mg/l), when compared to probable, possible infection groups and PJI unlikely group (8 mg/l, 8.3 mg/l, 3.6 mg/l, respectively, p < 0.05). The most common isolated microorganism was Cutibacterium acnes in 25 patients (48%) followed by coagulase-negative staphylococci (CNS) in 20 patients (39%). Patients with a PJI caused by high-virulent microorganisms had a significantly higher median serum CRP level compared to patients with PJI caused by low-virulent microorganisms (48 mg/l vs. 11.3 mg/l, p = 0.04).
Conclusions: Serum CRP showed a low sensitivity and specificity for the diagnosis of shoulder PJI, even applying cutoffs optimized by receiver-operating curve analysis. Low-virulent microorganisms and patients with probable and possible infections are associated with lower CRP levels compared to patients with definitive infection and infections caused by high-virulent microorganisms.
Level of evidence: Diagnostic Level III.
Keywords: C-reactive protein; Definition; Low-virulence; Periprosthetic shoulder infection.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Zmistowski B, Della Valle C, Bauer TW, Malizos KN, Alavi A, Bedair H, Booth RE, Choong P, Deirmengian C, Ehrlich GD, Gambir A, Huang R, Kissin Y, Kobayashi H, Kobayashi N, Krenn V, Drago L, Marston SB, Meermans G, Perez J, Ploegmakers JJ, Rosenberg A, Simpendorfer C, Thomas P, Tohtz S, Villafuerte JA, Wahl P, Wagenaar FC, Witzo E. Diagnosis of periprosthetic joint infection. J Arthroplasty. 2014;29:77–83. doi: 10.1016/j.arth.2013.09.040. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
