

In-hospital cardiac arrest in patients with coronavirus 2019
- PMID: 33515638
- PMCID: PMC7839632
- DOI: 10.1016/j.resuscitation.2021.01.012
In-hospital cardiac arrest in patients with coronavirus 2019
Abstract
Background: Coronavirus Disease 2019 (COVID-19) has caused over 1 200 000 deaths worldwide as of November 2020. However, little is known about the clinical outcomes among hospitalized patients with active COVID-19 after in-hospital cardiac arrest (IHCA).
Aim: We aimed to characterize outcomes from IHCA in patients with COVID-19 and to identify patient- and hospital-level variables associated with 30-day survival.
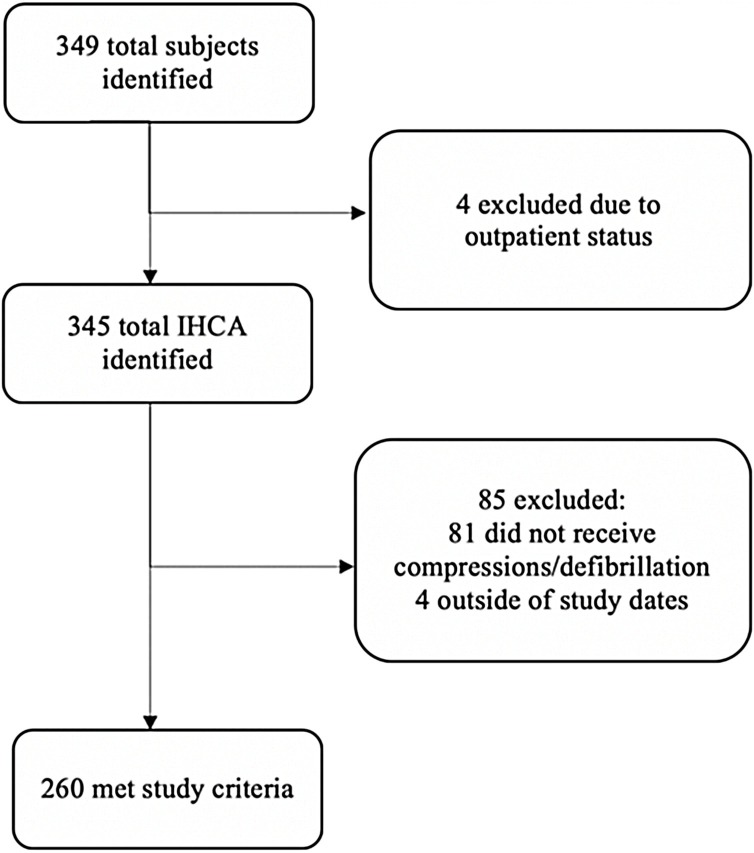
Methods: We conducted a multicentre retrospective cohort study across 11 academic medical centres in the U.S. Adult patients who received cardiopulmonary resuscitation and/or defibrillation for IHCA between March 1, 2020 and May 31, 2020 who had a documented positive test for Severe Acute Respiratory Syndrome Coronavirus 2 were included. The primary outcome was 30-day survival after IHCA.
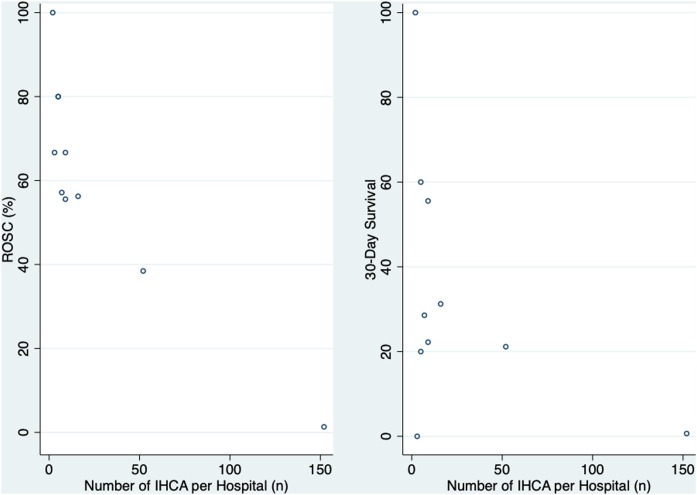
Results: There were 260 IHCAs among COVID-19 patients during the study period. The median age was 69 years (interquartile range 60-77), 71.5% were male, 49.6% were White, 16.9% were Black, and 16.2% were Hispanic. The most common presenting rhythms were pulseless electrical activity (45.0%) and asystole (44.6%). ROSC occurred in 58 patients (22.3%), 31 (11.9%) survived to hospital discharge, and 32 (12.3%) survived to 30 days. Rates of ROSC and 30-day survival in the two hospitals with the highest volume of IHCA over the study period compared to the remaining hospitals were considerably lower (10.8% vs. 64.3% and 5.9% vs. 35.7% respectively, p < 0.001 for both).
Conclusions: We found rates of ROSC and 30-day survival of 22.3% and 12.3% respectively. There were large variations in centre-level outcomes, which may explain the poor survival in prior studies.
Keywords: COVID-19; Cohort study; In-hospital cardiac arrest.
Copyright © 2021 Elsevier B.V. All rights reserved.
Figures
References
-
- Center for Systems Science and Engineering at Johns Hopkins Hospital . 2020. COVID-19 dashboard.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
