

Association of metformin monotherapy or combined therapy with cardiovascular risks in patients with type 2 diabetes mellitus
- PMID: 33516224
- PMCID: PMC7847575
- DOI: 10.1186/s12933-020-01202-5
Association of metformin monotherapy or combined therapy with cardiovascular risks in patients with type 2 diabetes mellitus
Abstract
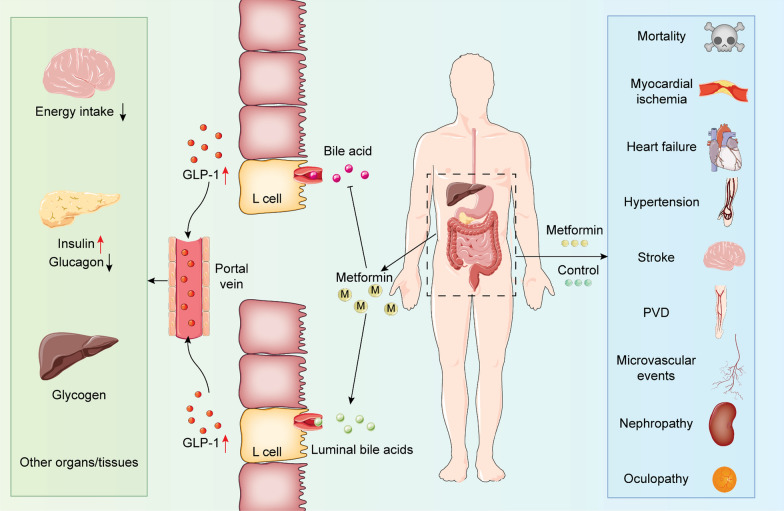
Background: Metformin is a first-line drug in type 2 diabetes mellitus (T2DM) treatment, yet whether metformin may increase all-cause or cardiovascular mortality of T2DM patients remains inconclusive.
Methods: We searched PubMed and Embase for data extracted from inception to July 14, 2020, with a registration in PROSPERO (CRD42020177283). This study included randomized controlled trials (RCT) assessing the cardiovascular effects of metformin for T2DM. This study is followed by PRISMA and Cochrane guideline. Risk ratio (RR) with 95% CI was pooled across trials by a random-effects model. Primary outcomes include all-cause mortality and cardiovascular mortality.
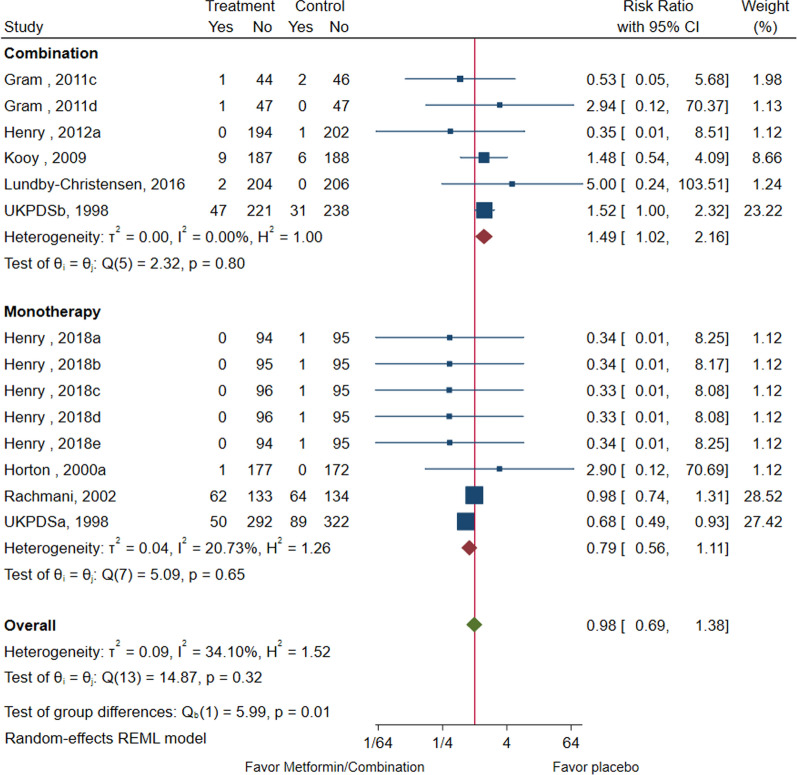
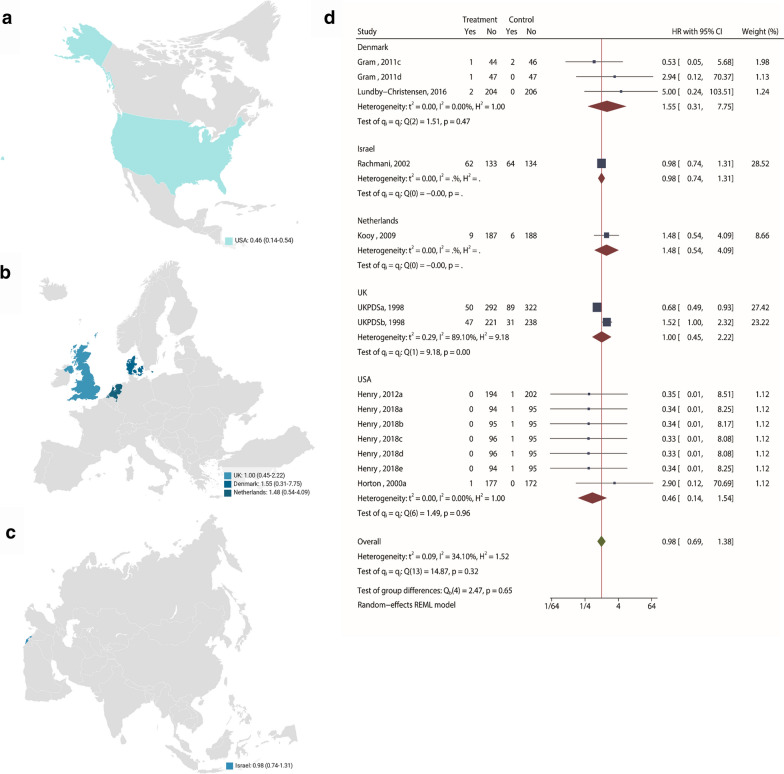
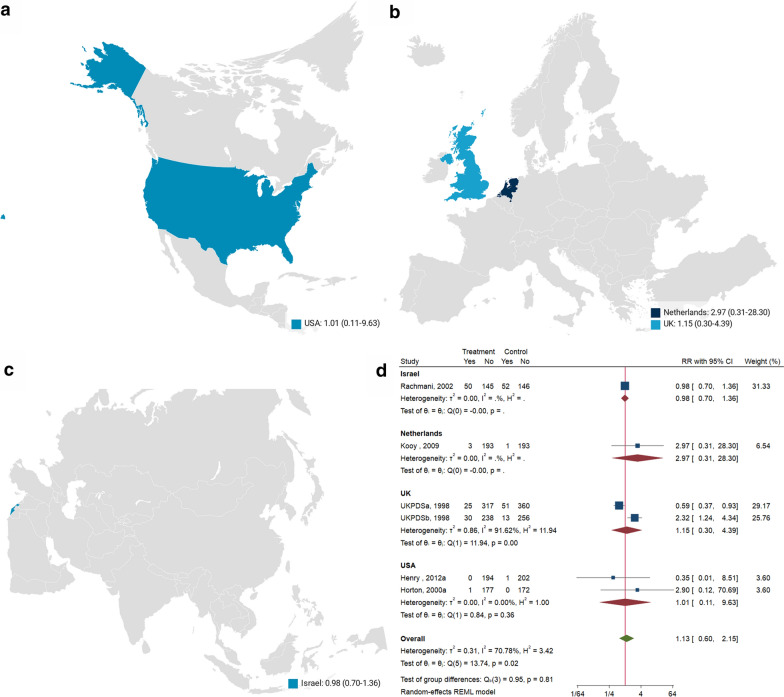
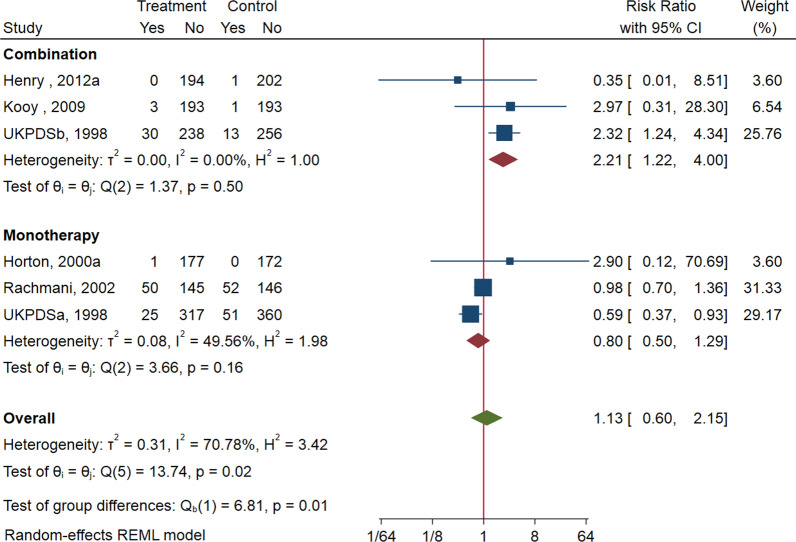
Results: We identified 29 studies that randomly assigned patients with 371 all-cause and 227 cardiovascular death events. Compared with untreated T2DM patients, metformin-treated patients was not associated with lower risk of all-cause mortality (RR: 0.98; 95%CI: 0.69-1.38; P = 0.90), cardiovascular mortality (RR: 1.13; 95% CI: 0.60, 2.15; P = 0.70), macrovascular events (RR: 0.87; 95%CI: 0.70-1.07; P = 0.19), heart failure (RR: 1.02; 95% CI:0.61-1.71; P = 0.95), and microvascular events (RR: 0.78; 95% CI:0.54-1.13; P = 0.19). Combination of metformin with another hypoglycemic drug was associated with higher risk of all-cause mortality (RR: 1.49; 95% CI: 1.02, 2.16) and cardiovascular mortality (RR: 2.21; 95% CI: 1.22, 4.00) compared with hypoglycemic drug regimens with no metformin.
Conclusion: The combination of metformin treatment may impose higher risk in all-cause and cardiovascular mortality. This finding, at least in part, shows no evidence for benefits of metformin in combination in terms of all-cause/cardiovascular mortality and cardiovascular events for T2DM. However, the conclusion shall be explained cautiously considering the limitations from UK Prospective Diabetes Study (UKPDS).
Keywords: Cardiovascular diseases; Metformin; Microvascular events; Mortality; Myocardial ischemia; Type 2 diabetes mellitus.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Das SR, et al. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation. 2019;139(10):e56–e528. doi: 10.1161/CIR.0000000000000659. - DOI - PubMed
-
- Inzucchi SE, Bergenstal RM, Buse JB, Diamant M, Ferrannini E, Nauck M, Peters AL, Tsapas A, Wender R, Matthews DR. Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2015;38(1):140–149. doi: 10.2337/dc14-2441. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
