

Associations between pre-pregnancy psychosocial risk factors and infant outcomes: a population-based cohort study in England
- PMID: 33516292
- PMCID: PMC7848754
- DOI: 10.1016/S2468-2667(20)30210-3
Associations between pre-pregnancy psychosocial risk factors and infant outcomes: a population-based cohort study in England
Abstract
Background: Existing studies evaluating the association between maternal risk factors and specific infant outcomes such as birthweight, injury admissions, and mortality have mostly focused on single risk factors. We aimed to identify routinely recorded psychosocial characteristics of pregnant women most at risk of adverse infant outcomes to inform targeting of early intervention.
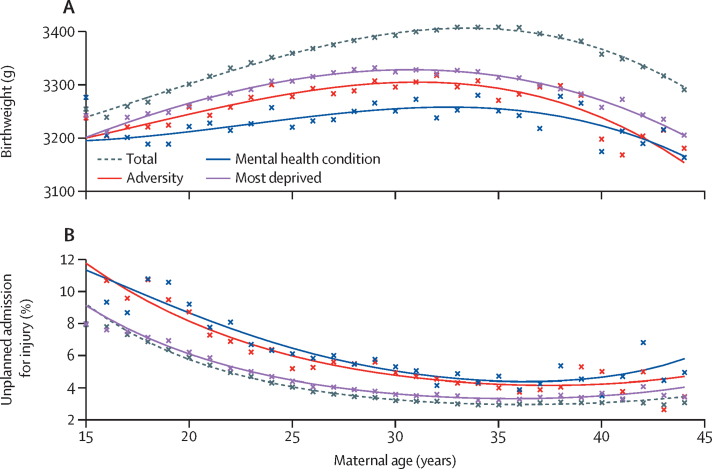
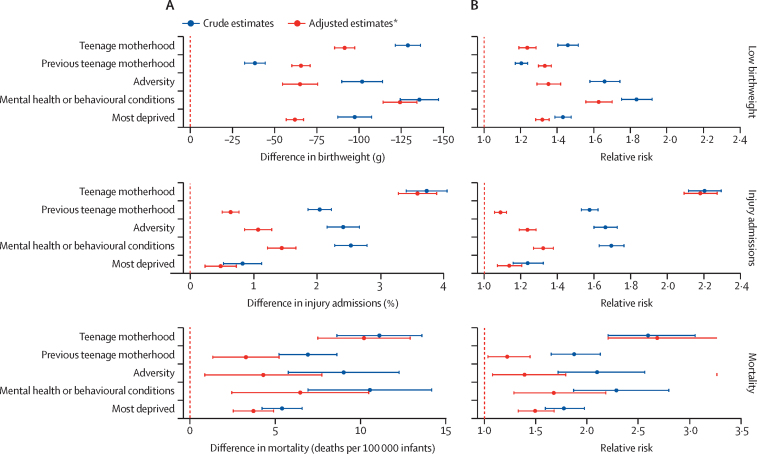
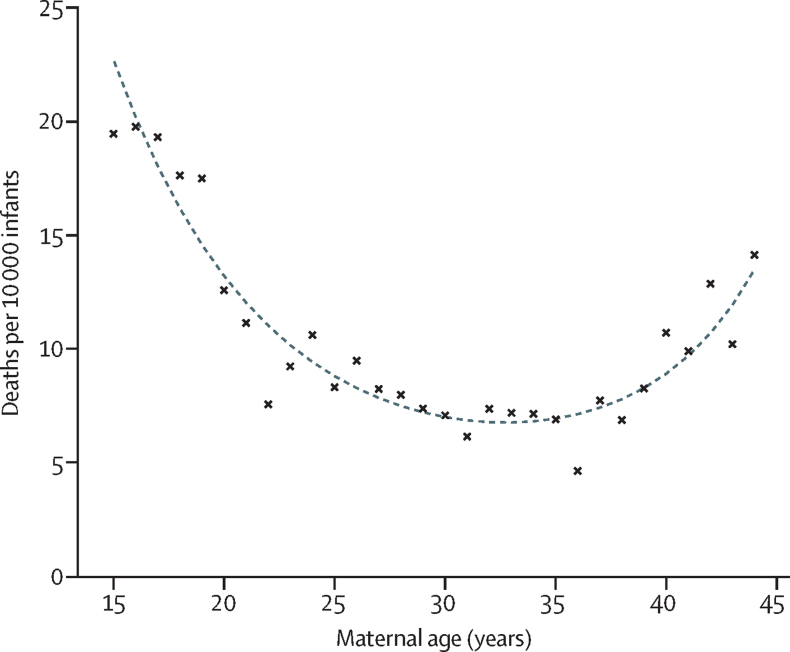
Methods: We created a cohort using administrative hospital data (Hospital Episode Statistics) for all births to mothers aged 15-44 years in England, UK, who gave birth on or after April 1, 2010, and who were discharged before or on March 31, 2015. We used generalised linear models to evaluate associations between psychosocial risk factors recorded in hospital records in the 2 years before the 20th week of pregnancy (ie, teenage motherhood, deprivation, pre-pregnancy hospital admissions for mental health or behavioural conditions, and pre-pregnancy hospital admissions for adversity, including drug or alcohol abuse, violence, and self-harm) and infant outcomes (ie, birthweight, unplanned admission for injury, or death from any cause, within 12 months from postnatal discharge).
Findings: Of 2 520 501 births initially assessed, 2 137 103 were eligible and were included in the birth outcome analysis. Among the eligible births, 93 279 (4·4%) were births to teenage mothers (age <20 years), 168 186 (7·9%) were births to previous teenage mothers, 51 312 (2·4%) were births to mothers who had a history of hospital admissions for mental health or behavioural conditions, 58 107 (2·7%) were births to mothers who had a history of hospital admissions for adversity, and 580 631 (27·2%) were births to mothers living in areas of high deprivation. 1 377 706 (64·5%) of births were to mothers with none of the above risk factors. Infants born to mothers with any of these risk factors had poorer outcomes than those born to mothers without these risk factors. Those born to mothers with a history of mental health or behavioural conditions were 124 g lighter (95% CI 114-134 g) than those born to mothers without these conditions. For teenage mothers compared with older mothers, 3·6% (95% CI 3·3-3·9%) more infants had an unplanned admission for injury, and there were 10·2 (95% CI 7·5-12·9) more deaths per 10 000 infants.
Interpretation: Health-care services should respond proactively to pre-pregnancy psychosocial risk factors. Our study demonstrates a need for effective interventions before, during, and after pregnancy to reduce the downstream burden on health services and prevent long-term adverse effects for children.
Funding: Wellcome Trust.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- National Institute of Clinical Excellence Pregnancy and complex social factors: a model for service provision for pregnant women with complex social factors. NICE guidelines CG110. 2010. https://www.nice.org.uk/guidance/cg110 - PubMed
-
- Murray AL, Kaiser D, Valdebenito S. The intergenerational effects of intimate partner violence in pregnancy: mediating pathways and implications for prevention. Trauma Violence Abuse. 2018;21:964–976. - PubMed
-
- Pierce M, Hope HF, Kolade A. Effects of parental mental illness on children's physical health: systematic review and meta-analysis. Br J Psychiatry. 2019;217:354–363. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
