

Improving long-term health outcomes of preterm infants: how to implement the findings of nutritional intervention studies into daily clinical practice
- PMID: 33517483
- PMCID: PMC8105221
- DOI: 10.1007/s00431-021-03950-2
Improving long-term health outcomes of preterm infants: how to implement the findings of nutritional intervention studies into daily clinical practice
Abstract
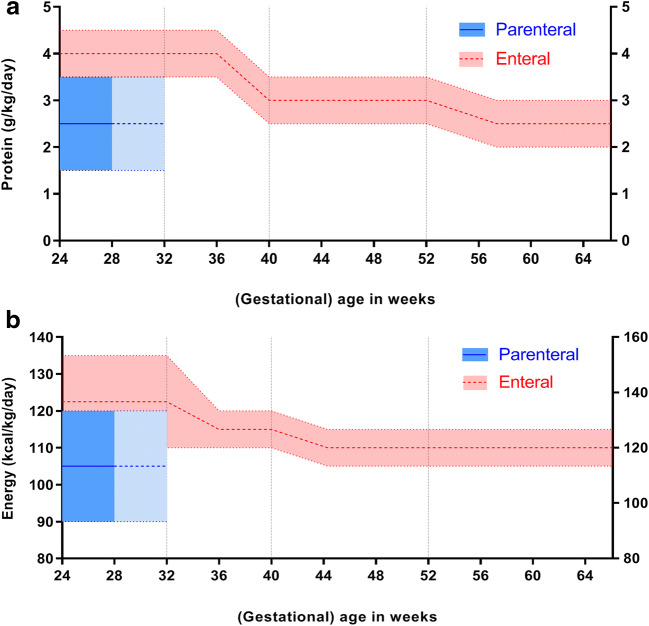
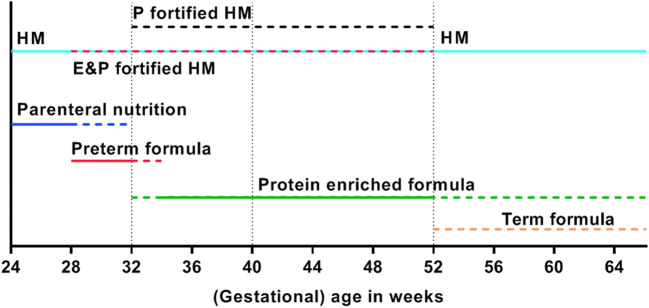
Preterm-born children are at risk for later neurodevelopmental problems and cardiometabolic diseases; early-life growth restriction and suboptimal neonatal nutrition have been recognized as risk factors. Prevention of these long-term sequelae has been the focus of intervention studies. High supplies of protein and energy during the first weeks of life (i.e., energy > 100 kcal kg-1 day-1 and a protein-to-energy ratio > 3 g/100 kcal) were found to improve both early growth and later neurodevelopmental outcome. Discontinuation of this high-energy diet is advised beyond 32-34 weeks postconceptional age to prevent excess fat mass and possible later cardiometabolic diseases. After discharge, nutrition with a higher protein-to-energy ratio (i.e., > 2.5-3.0 g/100 kcal) may improve growth and body composition in the short term.Conclusion: Preterm infants in their first weeks of life require a high-protein high-energy diet, starting shortly after birth. Subsequent adjustments in nutritional composition, aimed at achieving optimal body composition and minimizing the long-term cardiometabolic risks without jeopardizing the developing brain, should be guided by the growth pattern. The long-term impact of this strategy needs to be studied. What is Known: • Preterm infants are at risk for nutritional deficiencies and extrauterine growth restriction. • Extrauterine growth restriction and suboptimal nutrition are risk factors for neurodevelopmental problems and cardiometabolic disease in later life. What is New: • Postnatally, a shorter duration of high-energy nutrition may prevent excess fat mass accretion and its associated cardiometabolic risks and an early switch to a protein-enriched diet should be considered from 32-34 weeks postconceptional age. • In case of formula feeding, re-evaluate the need for the continuation of a protein-enriched diet, based on the infant's growth pattern.
Keywords: Early nutrition; Postnatal growth restriction; Preterm birth; Protein-to-energy ratio.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller AB, Narwal R, Adler A, Vera Garcia C, Rohde S, Say L, Lawn JE. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379:2162–2172. - PubMed
-
- Shah PS, Lui K, Sjors G, Mirea L, Reichman B, Adams M, Modi N, Darlow BA, Kusuda S, San Feliciano L, Yang J, Hakansson S, Mori R, Bassler D, Figueras-Aloy J, Lee SK. Neonatal outcomes of very low birth weight and very preterm neonates: an international comparison. J Pediatr. 2016;177:144–152. - PubMed
-
- Stoll BJ, Hansen NI, Bell EF, Walsh MC, Carlo WA, Shankaran S, Laptook AR, Sanchez PJ, Van Meurs KP, Wyckoff M, Das A, Hale EC, Ball MB, Newman NS, Schibler K, Poindexter BB, Kennedy KA, Cotten CM, Watterberg KL, D’Angio CT, DeMauro SB, Truog WE, Devaskar U, Higgins RD. Trends in care practices, morbidity, and mortality of extremely preterm neonates, 1993-2012. Jama. 2015;314:1039–1051. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
