

COVID-19 pneumonia-ultrasound, radiographic, and computed tomography findings: a comprehensive pictorial essay
- PMID: 33517546
- PMCID: PMC7847301
- DOI: 10.1007/s10140-021-01905-6
COVID-19 pneumonia-ultrasound, radiographic, and computed tomography findings: a comprehensive pictorial essay
Abstract
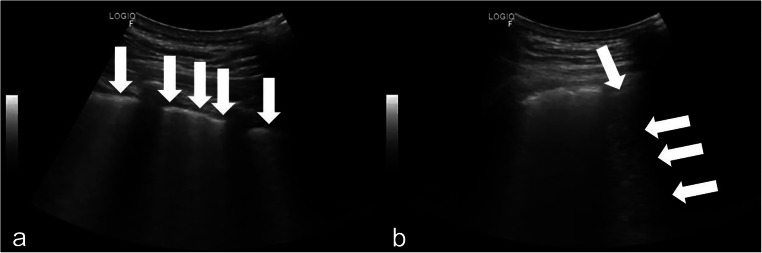
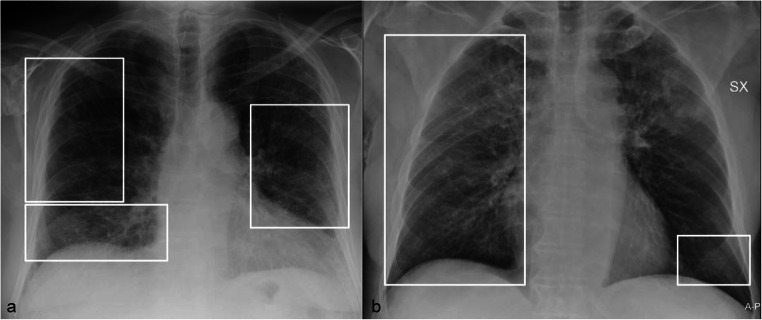
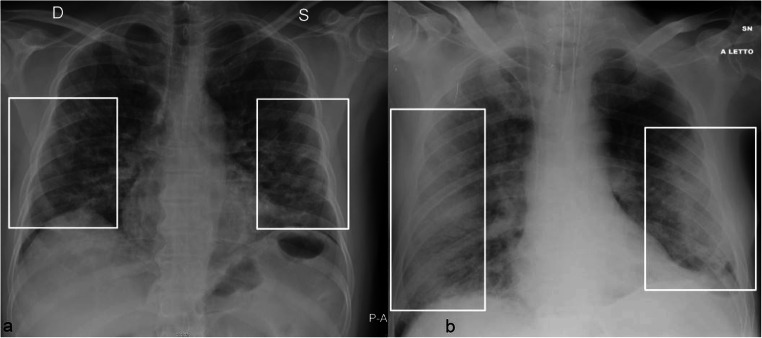
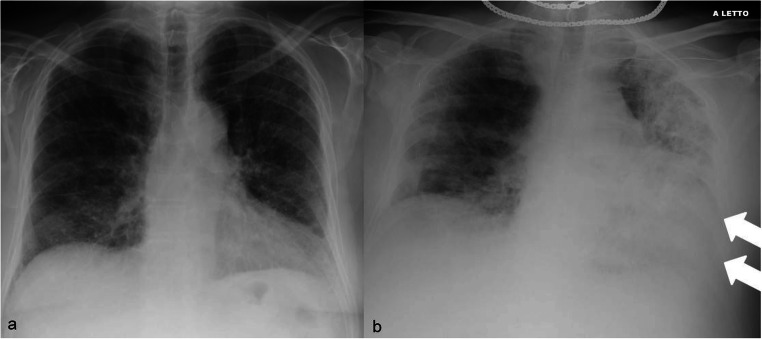
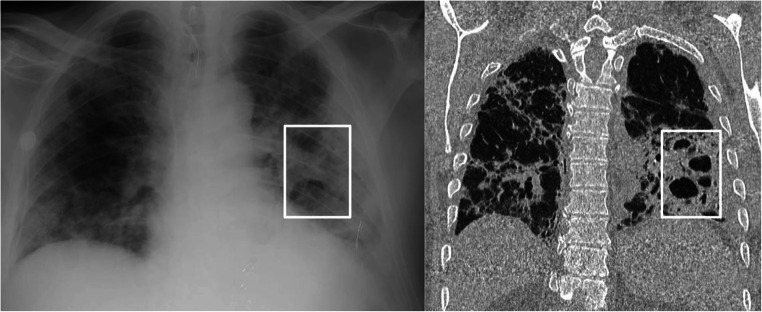
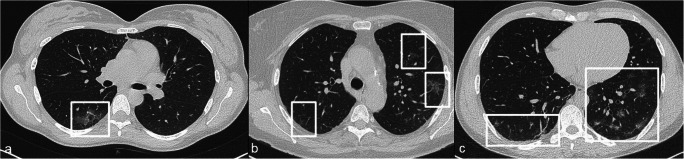
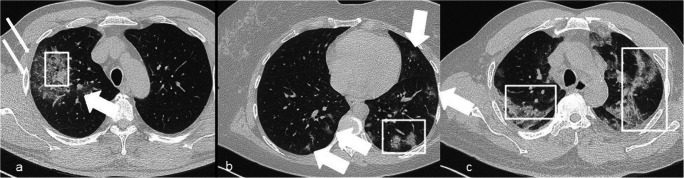
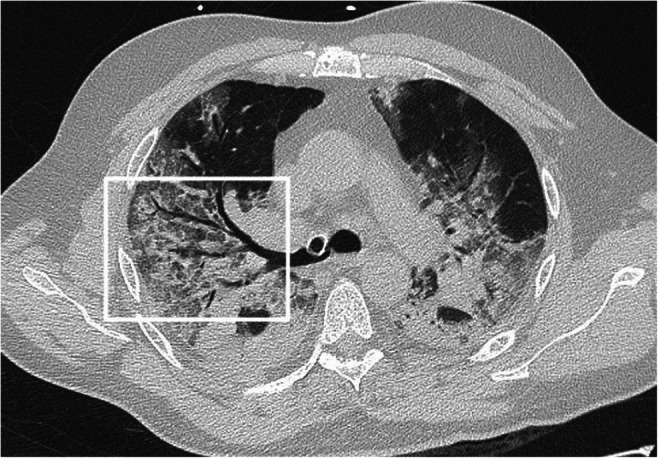
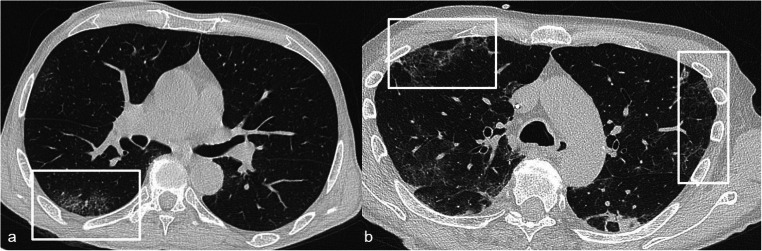
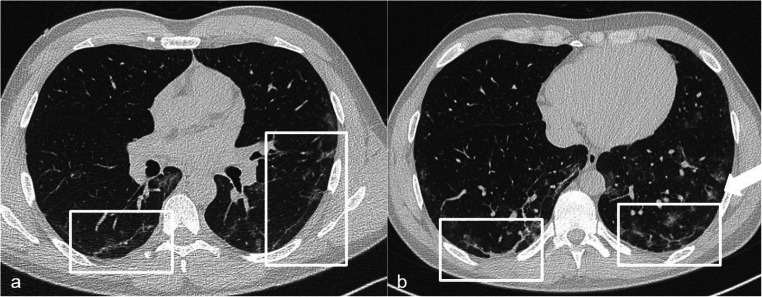
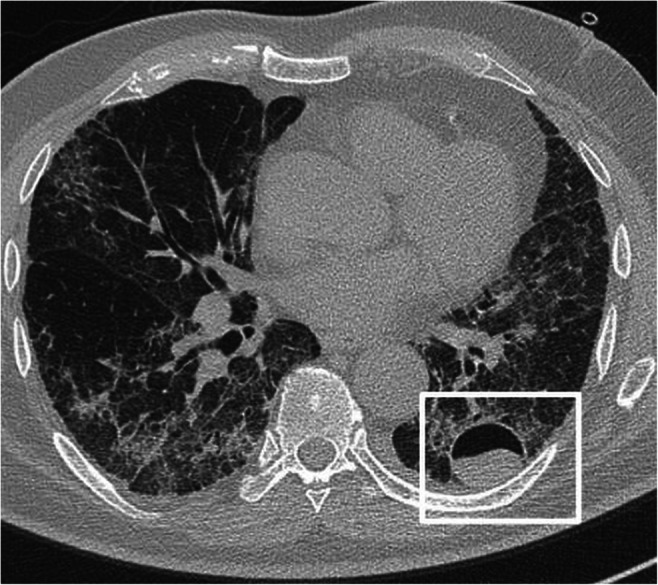
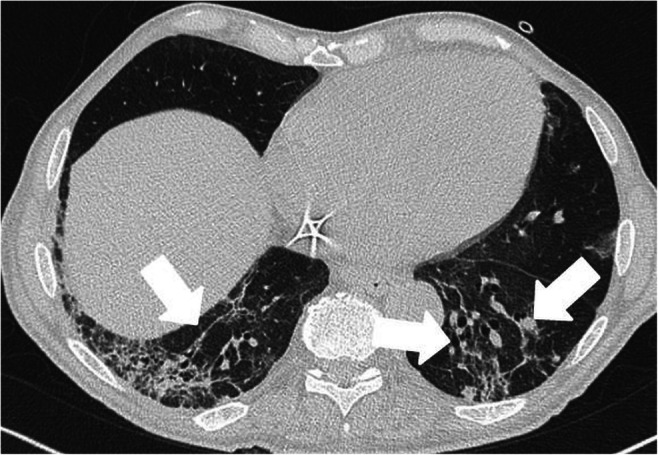
Ultrasound, chest X-ray, and computed tomography (CT) have been used with excellent results in diagnosis, first assessment, and follow-up of COVID-19 confirmed and suspected patients. Ultrasound and chest X-ray have the advantages of the wide availability and acquisition at the patient's bed; CT showed high sensitivity in COVID-19 diagnosis. Ground-glass opacities and consolidation are the main CT and X-ray features; the distribution of lung abnormalities is typically bilateral and peripheral. Less typical findings, including pleural effusion, mediastinal lymphadenopathies, the bubble air sign, and cavitation, can also be visible on chest CT. Radiologists should be aware of the advantages and limitations of the available imaging techniques and of the different pulmonary aspects of COVID-19 infection.
Keywords: COVID-19; Coronavirus; Pneumonia, viral; Severe acute respiratory syndrome coronavirus 2; Tomography, spiral computed.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

Similar articles
-
Chest computed tomography findings of COVID-19 pneumonia: pictorial essay with literature review.Jpn J Radiol. 2020 Nov;38(11):1012-1019. doi: 10.1007/s11604-020-01010-7. Epub 2020 Jun 25. Jpn J Radiol. 2020. PMID: 32588277 Free PMC article. Review.
-
Correlation between Chest Computed Tomography and Lung Ultrasonography in Patients with Coronavirus Disease 2019 (COVID-19).Ultrasound Med Biol. 2020 Nov;46(11):2918-2926. doi: 10.1016/j.ultrasmedbio.2020.07.003. Epub 2020 Jul 13. Ultrasound Med Biol. 2020. PMID: 32771222 Free PMC article.
-
Thoracic imaging tests for the diagnosis of COVID-19.Cochrane Database Syst Rev. 2020 Sep 30;9:CD013639. doi: 10.1002/14651858.CD013639.pub2. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2020 Nov 26;11:CD013639. doi: 10.1002/14651858.CD013639.pub3. PMID: 32997361 Updated.
-
Imaging and clinical features of patients with 2019 novel coronavirus SARS-CoV-2.Eur J Nucl Med Mol Imaging. 2020 May;47(5):1275-1280. doi: 10.1007/s00259-020-04735-9. Epub 2020 Feb 28. Eur J Nucl Med Mol Imaging. 2020. PMID: 32107577 Free PMC article.
-
Radiology of COVID-19 - Imaging the pulmonary damage.J Pak Med Assoc. 2020 May;70(Suppl 3)(5):S60-S63. doi: 10.5455/JPMA.21. J Pak Med Assoc. 2020. PMID: 32515387
Cited by
-
Role of Artificial Intelligence in COVID-19 Detection.Sensors (Basel). 2021 Dec 1;21(23):8045. doi: 10.3390/s21238045. Sensors (Basel). 2021. PMID: 34884045 Free PMC article.
-
COVID-19 and Lung Cavitation: A Clue to Pathogenesis?HCA Healthc J Med. 2022 Aug 29;3(4):253-256. doi: 10.36518/2689-0216.1361. eCollection 2022. HCA Healthc J Med. 2022. PMID: 37426868 Free PMC article.
-
The diagnostic performance of automatic B-lines detection for evaluating pulmonary edema in the emergency department among novice point-of-care ultrasound practitioners.Emerg Radiol. 2025 Apr;32(2):241-246. doi: 10.1007/s10140-025-02319-4. Epub 2025 Feb 14. Emerg Radiol. 2025. PMID: 39951213 Free PMC article.
-
Deep CNN models for predicting COVID-19 in CT and x-ray images.J Med Imaging (Bellingham). 2021 Jan;8(Suppl 1):014502. doi: 10.1117/1.JMI.8.S1.014502. Epub 2021 Apr 21. J Med Imaging (Bellingham). 2021. PMID: 33912622 Free PMC article.
-
Pixel-based analysis of pulmonary changes on CT lung images due to COVID-19 pneumonia.J Clin Imaging Sci. 2022 Feb 19;12:6. doi: 10.25259/JCIS_172_2021. eCollection 2022. J Clin Imaging Sci. 2022. PMID: 35251762 Free PMC article.
References
-
- Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, Zhao X, Huang B, Shi W, Lu R, Niu P, Zhan F, Ma X, Wang D, Xu W, Wu G, Gao GF, Tan W (2020) China novel coronavirus investigating and research team. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med20;382(8):727-733. 10.1056/NEJMoa2001017 - PubMed
-
- WHO Coronavirus disease (COVID-19) dashboard. https://covid19.who.int/ accessed November 22
-
- Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, Liu L, Shan H, Lei CL, Hui DSC, Du B, Li LJ, Zeng G, Yuen KY, Chen RC, Tang CL, Wang T, Chen PY, Xiang J, Li SY, Wang JL, Liang ZJ, Peng YX, Wei L, Liu Y, Hu YH, Peng P, Wang JM, Liu JY, Chen Z, Li G, Zheng ZJ, Qiu SQ, Luo J, Ye CJ, Zhu SY, Zhong NS (2020) China medical treatment expert group for Covid-19. Clinical characteristics of coronavirus disease 2019 in China. N Engl J med 30;382(18):1708-1720. 10.1056/NEJMoa2002032 - PMC - PubMed
-
- Hu Z, Song C, Xu C, Jin G, Chen Y, Xu X, Ma H, Chen W, Lin Y, Zheng Y, Wang J, Hu Z, Yi Y, Shen H. Clinical characteristics of 24 asymptomatic infections with COVID-19 screened among close contacts in Nanjing, China. Sci China Life Sci. 2020;63(5):706–711. doi: 10.1007/s11427-020-1661-4. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
