

[18F]FDG PET/MRI in rectal cancer
- PMID: 33517562
- PMCID: PMC7902586
- DOI: 10.1007/s12149-021-01580-0
[18F]FDG PET/MRI in rectal cancer
Abstract
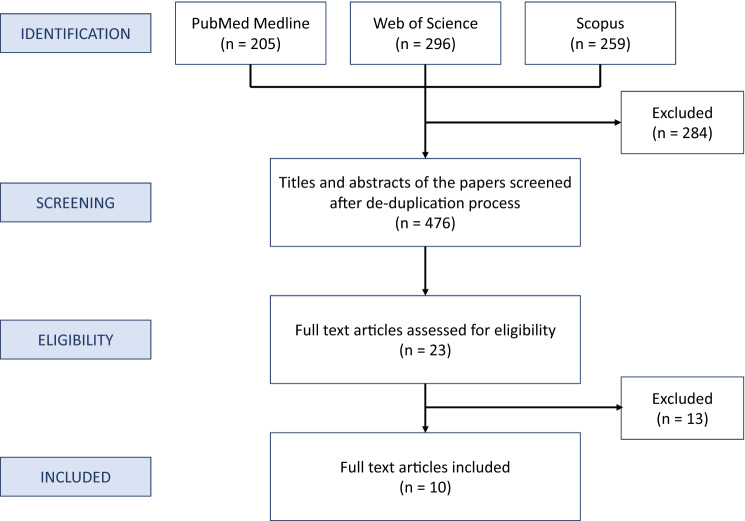
We conducted a systematic literature review on the use of [18F]FDG PET/MRI for staging/restaging rectal cancer patients with PubMed, Scopus, and Web of Science, based on the PRISMA criteria. Three authors screened all titles and abstracts and examined the full texts of all the identified relevant articles. Studies containing aggregated or duplicated data, review articles, case reports, editorials, and letters were excluded. Ten reports met the inclusion criteria. Four studies examined T staging and one focused on local recurrences after surgery; the reported sensitivity (94-100%), specificity (73-94%), and accuracy (92-100%) varied only slightly from one study to another. The sensitivity, specificity, and accuracy of [18F]FDG PET/MRI for N staging were 90-93%, 92-94%, and 42-92%. [18F]FDG PET/MRI detected malignant nodes better than MRI, resulting in treatment change. For M staging, [18F]FDG PET/MRI outperformed [18F]FDG PET/CT and CT in detecting liver metastases, whereas it performed worse for lung metastases. The results of this review suggest that [18F]FDG PET/MRI should be used for rectal cancer restaging after chemoradiotherapy and to select patients for rectum-sparing approaches thanks to its accuracy in T and N staging. For M staging, it should be associated at least with a chest CT scan to rule out lung metastases.
Keywords: PET/MRI; Rectal cancer; [18F]FDG.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Amin MB, Greene FL, Edge SB, Compton CC, Gershenwald JE, Brookland RK, et al. The eighth edition AJCC Cancer Staging Manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67:93–99. doi: 10.3322/caac.21388. - DOI - PubMed
-
- Ma B, Gao P, Wang H, Xu Q, Song Y, Huang X, et al. What has preoperative radio(chemo)therapy brought to localized rectal cancer patients in terms of perioperative and long-term outcomes over the past decades? A systematic review and meta-analysis based on 41,121 patients. Int J Cancer. 2017;141:1052–1065. doi: 10.1002/ijc.30805. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
