

Sequential occurrence of microscopic polyangiitis and anti-glomerular basement membrane disease in a patient with small cell lung cancer: a case report
- PMID: 33517889
- PMCID: PMC7849101
- DOI: 10.1186/s13256-020-02614-3
Sequential occurrence of microscopic polyangiitis and anti-glomerular basement membrane disease in a patient with small cell lung cancer: a case report
Abstract
Background: The association between a preceding malignancy and the onset of anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) has been reported in several studies. While the co-existence of ANCA and anti-glomerular basement membrane (GBM) antibodies in an individual patient is not a common occurrence, this double-positive disease currently has no optimal treatment method. Herein, we report a case of a double-positive disease involving the sequential development of acute kidney injury (AKI) and diffuse alveolar hemorrhage (DAH) in a patient with small cell lung cancer (SCLC).
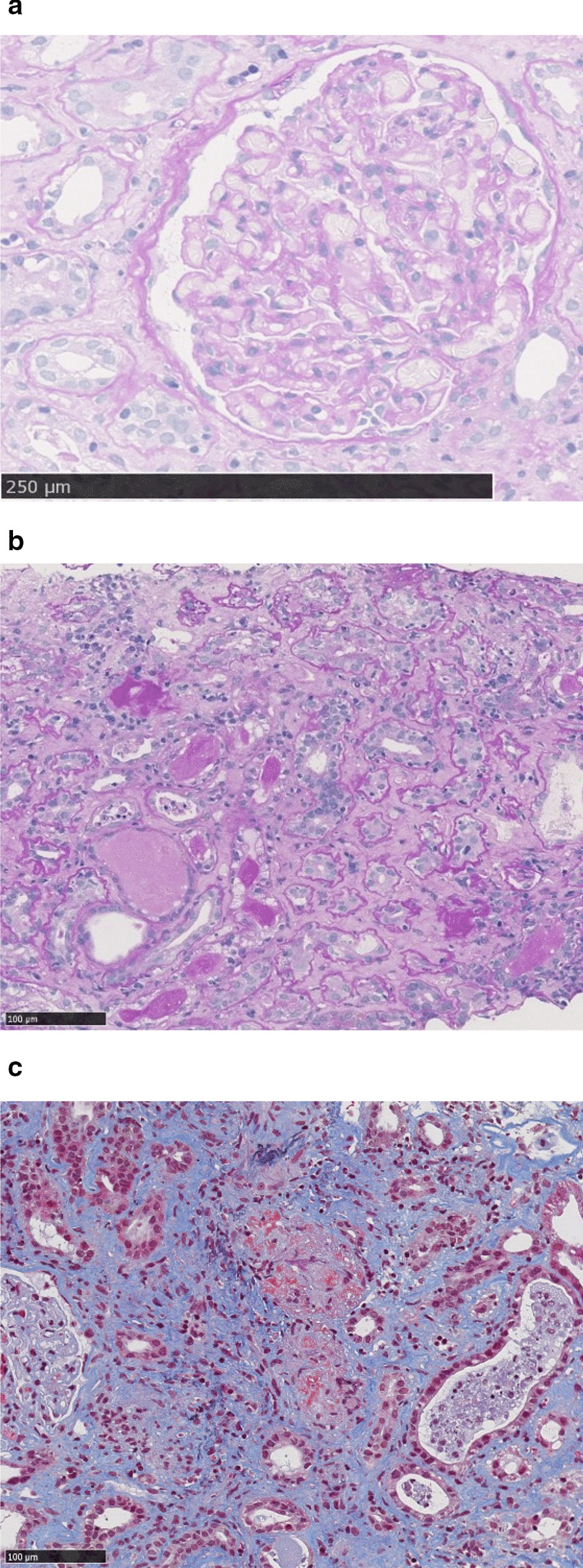
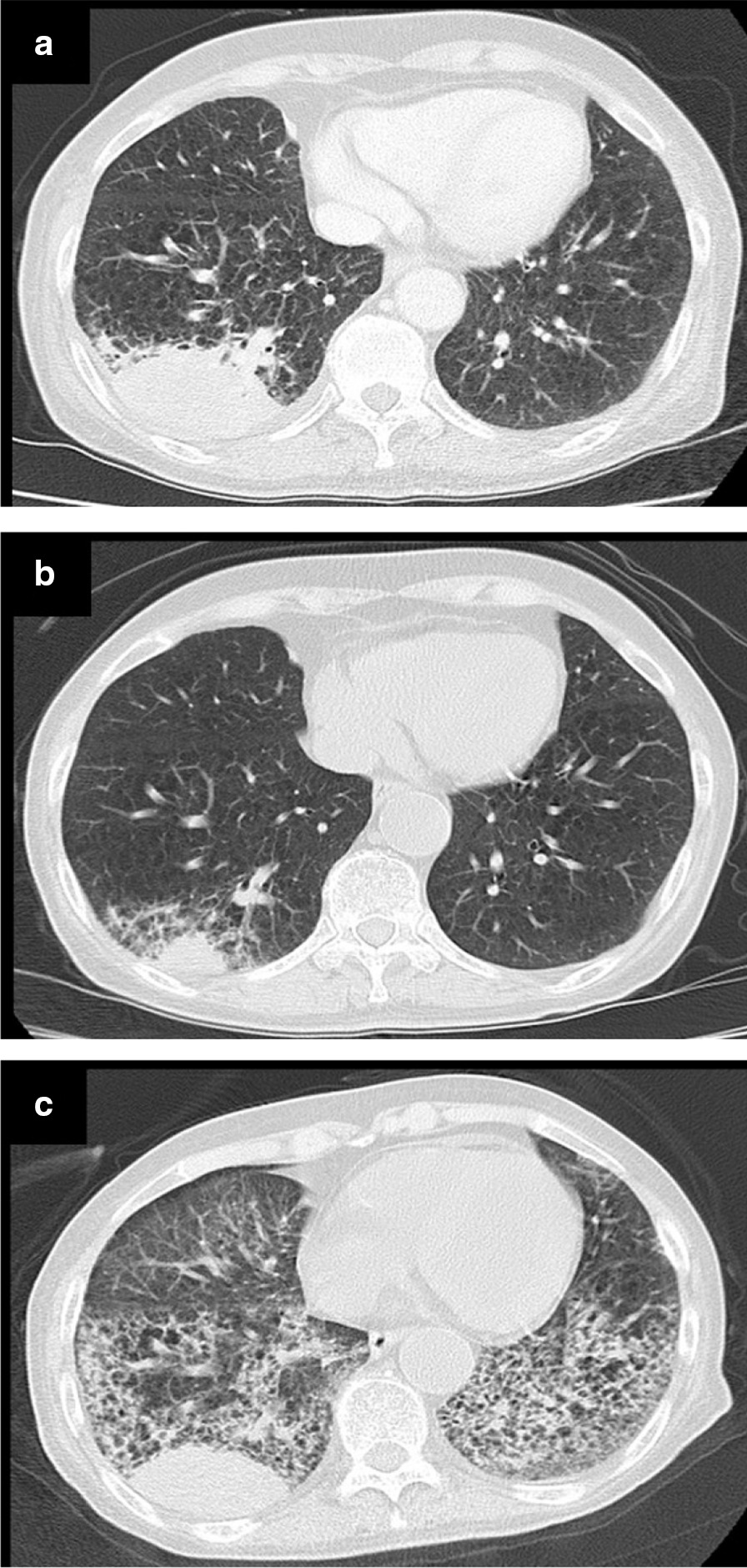
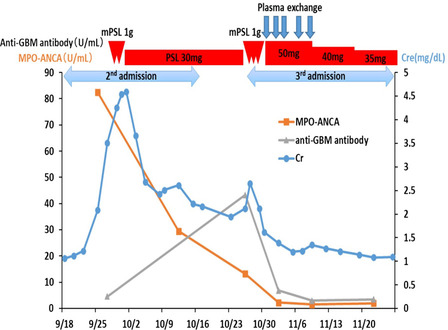
Case presentation: A 75-year-old Japanese woman was diagnosed with small cell lung cancer (cT3N2M1b cStage IV) and received chemotherapy. After one cycle of chemotherapy, she experienced fever and malaise. Her serum creatinine level rapidly increased, and she tested positive for myeloperoxidase (MPO)-ANCA and anti-GBM antibody. She was diagnosed with AKI due to microscopic polyangiitis (MPA) based on renal biopsy. Corticosteroid therapy was initiated, which improved her renal dysfunction. Eight days after she was discharged from the hospital, she complained of dyspnea and bloody sputum, and her condition rapidly progressed to respiratory failure. Upon chest imaging, ground-glass opacities were seen in her bilateral lower lungs. Laboratory examinations after admission revealed a lower MPO-ANCA titer and an elevated anti-GBM antibody titer compared to her previous admission. We diagnosed her with DAH due to an anti-GBM disease. After corticosteroid pulse therapy, plasma exchange was performed five times; her oxygen saturation and chest radiologic findings improved gradually. Following five cycles of plasma exchange, her oxygen saturation recovered to 95% in room air.
Conclusions: To our knowledge, this is the first reported case of vasculitis caused by MPA and anti-GBM disease leading to the development of AKI and DAH during treatment of SCLC. SCLC, MPA, and anti-GBM disease may occur sequentially. A double-positive disease might have a worse prognosis; therefore, intensive therapy is more likely to achieve a better outcome.
Keywords: Anti-glomerular basement membrane disease; Double-positive disease; Microscopic polyangiitis; Small cell lung cancer.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Short AK, Esnault VL, Lockwood CM. Anti-neutrophil cytoplasm antibodies and anti-glomerular basement membrane antibodies: two coexisting distinct autoreactivities detectable in patients with rapidly progressive glomerulonephritis. Am J Kidney Dis. 1995;26:439–445. doi: 10.1016/0272-6386(95)90489-1. - DOI - PubMed
-
- McAdoo SP, Tanna A, Hrušková Z, Holm L, Weiner M, Arulkumaran N, et al. Patients double-seropositive for ANCA and anti-GBM antibodies have varied renal survival, frequency of relapse, and outcomes compared to single-seropositive patients. Kidney Int. 2017;92:693–702. doi: 10.1016/j.kint.2017.03.014. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
