

Review
doi: 10.1016/j.ecl.2020.10.002.
Diagnosis of Polycystic Ovary Syndrome: Which Criteria to Use and When?
Affiliations
- PMID: 33518179
- PMCID: PMC7860982
- DOI: 10.1016/j.ecl.2020.10.002
Item in Clipboard
Review
Diagnosis of Polycystic Ovary Syndrome: Which Criteria to Use and When?
Endocrinol Metab Clin North Am.
2021 Mar.
Abstract
Current diagnostic criteria for polycystic ovary syndrome (PCOS) are based on expert opinion. This article reviews the rationale for and the limitations of these criteria as well as which criteria to use and when. The insights provided into PCOS pathogenesis by modern genetic analyses and the promise of objective data mining approaches for biologically relevant disease classification are discussed.
Keywords: Diagnostic criteria; Disease classification; Hyperandrogenism; PCOS; Polycystic ovary syndrome.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure The authors have nothing to disclose.
Figures
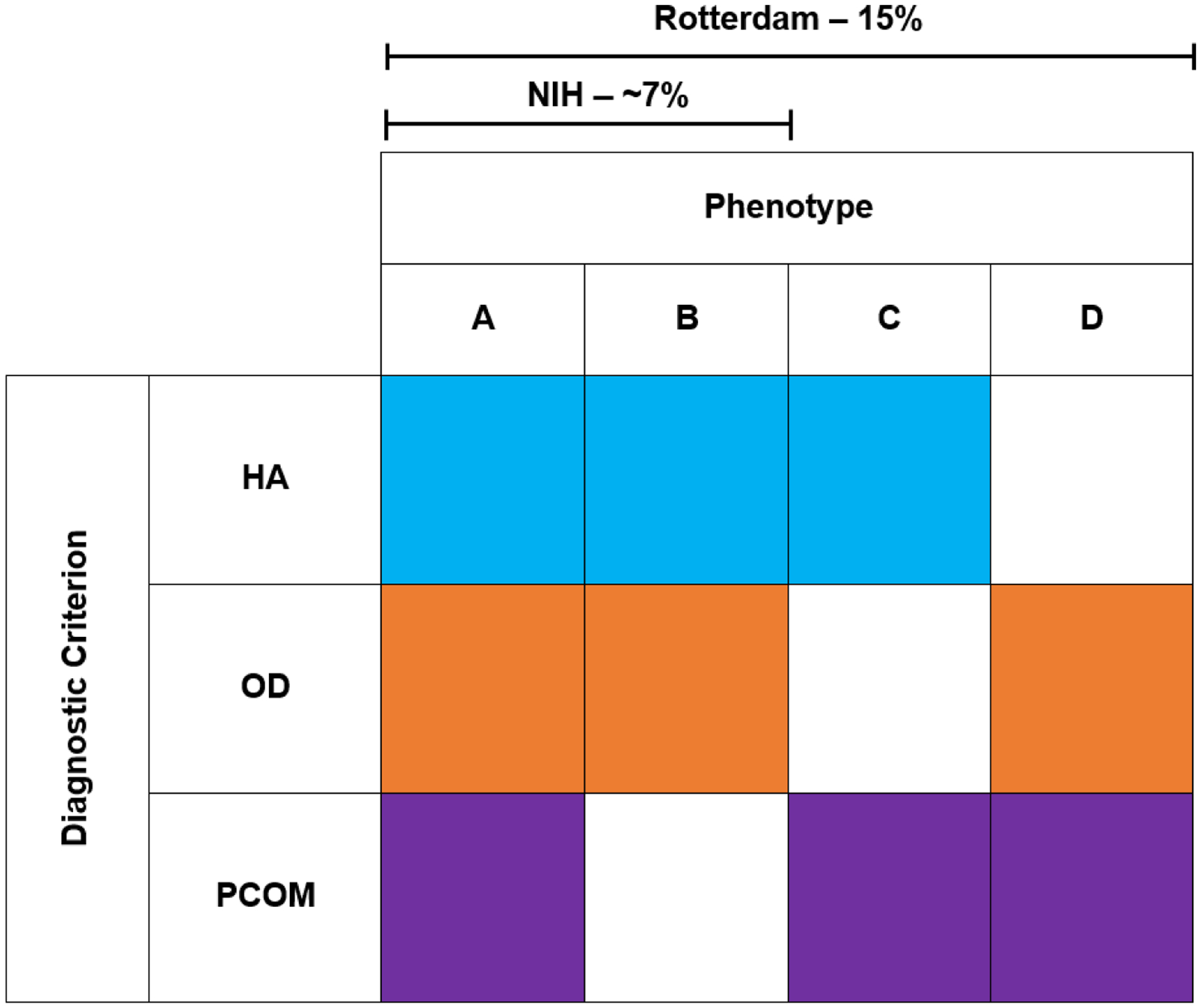
NIH PCOS must include both HA+OD, +/− PCOM. There are no endocrine or metabolic differences between phenotypes A and B; there is no need to assess PCOM in NIH PCOS. Rotterdam Criteria requires at least 2 out of the 3 criteria to be present, adding 2 new phenotypes HA+PCOM and OD+PCOM. The prevalence of PCOS increases from ~7% to 15% when including the two non-NIH Rotterdam phenotypes.
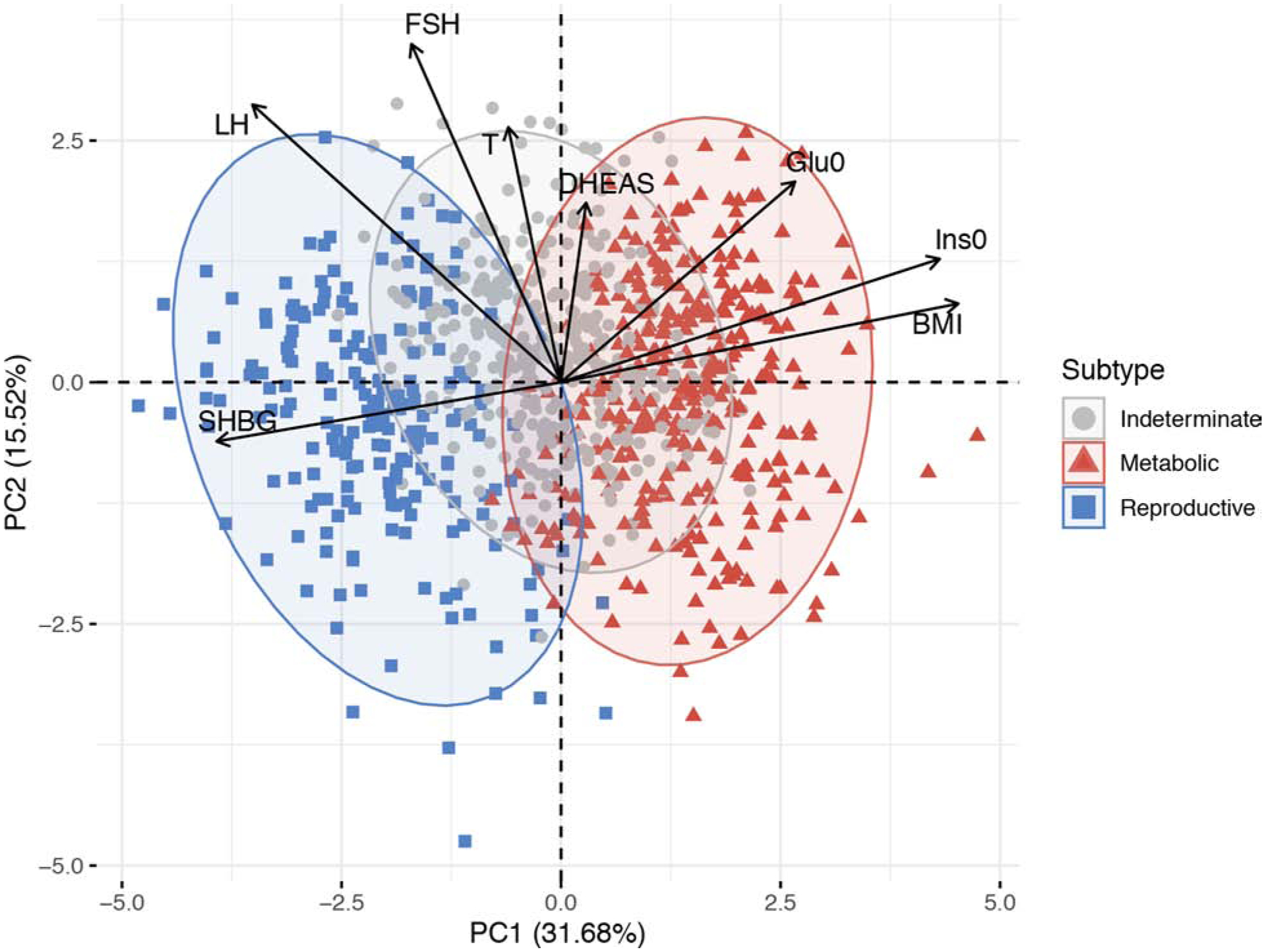
Women with PCOS were clustered into distinct groups—metabolic, reproductive, and indeterminate—based on BMI, fasting insulin, fasting glucose, DHEAS, T, FSH, LH, SHBG, and genotype data. The relative magnitude and direction of trait correlations with the principal components are shown with black arrows. PC=principal component; Ins0= fasting insulin; Glu0= fasting glucose. (From Dapas M, Lin FTJ, Nadkarni GN, et al. Distinct subtypes of polycystic ovary syndrome with novel genetic associations: An unsupervised, phenotypic clustering analysis. PLoS Med. 2020;17(6):e1003132; with permission.)
References
-
- Carmina E, Lobo RA. Polycystic ovary syndrome (PCOS): arguably the most common endocrinopathy is associated with significant morbidity in women. J Clin Endocrinol Metab. June 1999;84(6):1897–9. - PubMed
-
- Rubin KH, Glintborg D, Nybo M, Abrahamsen B, Andersen M. Development and Risk Factors of Type 2 Diabetes in a Nationwide Population of Women With Polycystic Ovary Syndrome. J Clin Endocrinol Metab. 10 2017;102(10):3848–3857. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
