

Pulmonary Vascular Thrombosis in COVID-19 Pneumonia
- PMID: 33518461
- PMCID: PMC7836419
- DOI: 10.1053/j.jvca.2021.01.011
Pulmonary Vascular Thrombosis in COVID-19 Pneumonia
Abstract
Objectives: During severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection, dramatic endothelial cell damage with pulmonary microvascular thrombosis have been was hypothesized to occur. The aim was to assess whether pulmonary vascular thrombosis (PVT) is due to recurrent thromboembolism from peripheral deep vein thrombosis or to local inflammatory endothelial damage, with a superimposed thrombotic late complication.
Design: Observational study.
Setting: Medical and intensive care unit wards of a teaching hospital.
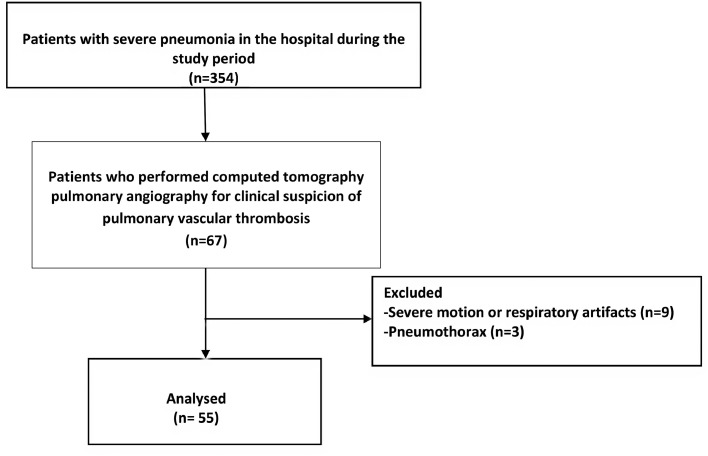
Participants: The authors report a subset of patients included in a prospective institutional study (CovidBiob study) with clinical suspicion of pulmonary vascular thromboembolism.
Interventions: Computed tomography pulmonary angiography and evaluation of laboratory markers and coagulation profile.
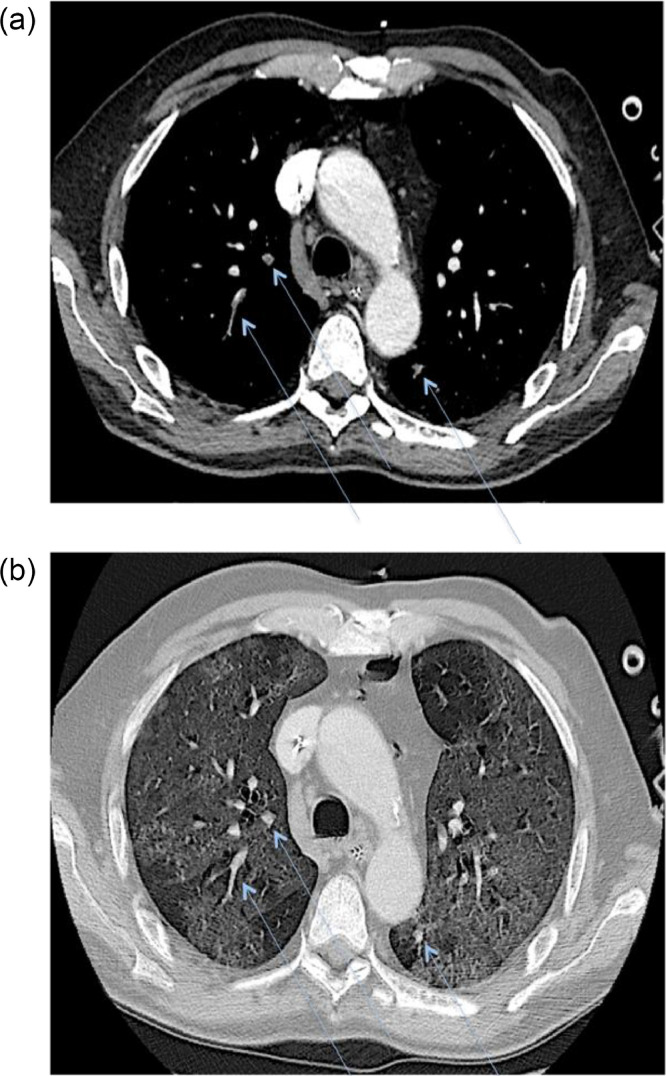
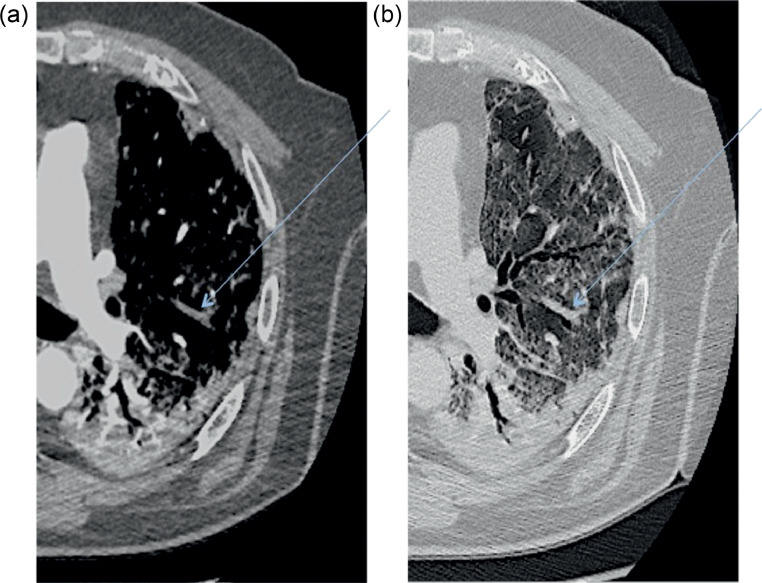
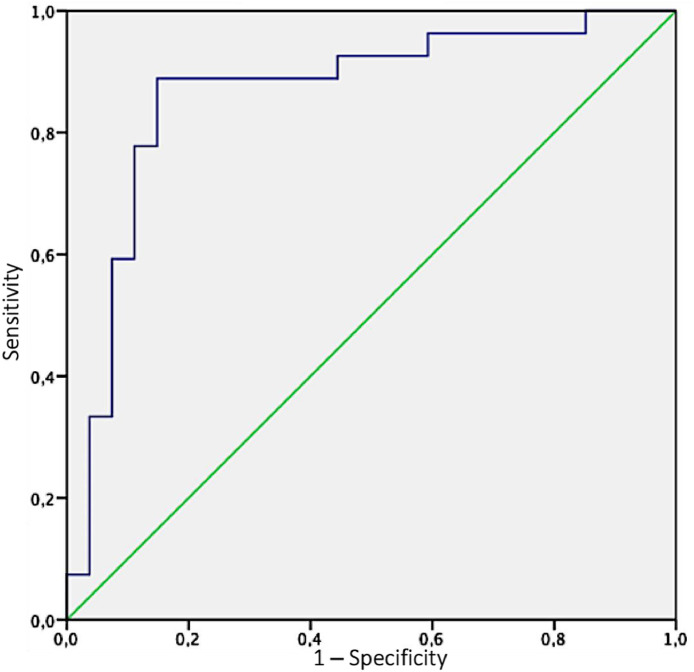
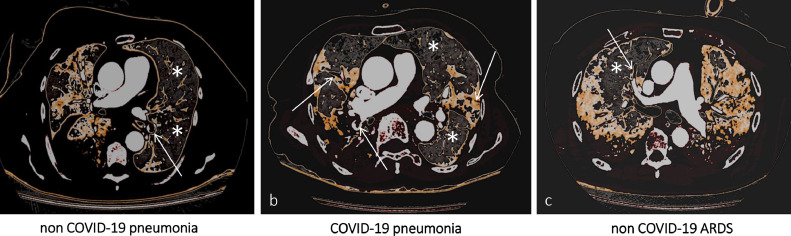
Measurements and main results: Twenty-eight of 55 (50.9%) patients showed PVT, with a median time interval from symptom onset of 17.5 days. Simultaneous multiple PVTs were identified in 22 patients, with bilateral involvement in 16, mostly affecting segmental/subsegmental pulmonary artery branches (67.8% and 96.4%). Patients with PVT had significantly higher ground glass opacity areas (31.7% [22.9-41] v 17.8% [10.8-22.1], p < 0.001) compared with those without PVT. Remarkably, in all 28 patients, ground glass opacities areas and PVT had an almost perfect spatial overlap. D-dimer level at hospital admission was predictive of PVT.
Conclusions: The findings identified a specific radiologic pattern of coronavirus disease 2019 (COVID-19) pneumonia with a unique spatial distribution of PVT overlapping areas of ground-glass opacities. These findings supported the hypothesis of a pathogenetic relationship between COVID-19 lung inflammation and PVT and challenged the previous definition of pulmonary embolism associated with COVID-19 pneumonia.
Keywords: COVID-19; D-dimer increase; computed tomography; critical care; inflammation; thrombosis.
Copyright © 2021 Elsevier Inc. All rights reserved.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
