

Cardiac Metastasis Caused Fatal Ventricular Arrhythmia in a Patient with a Rectal Neuroendocrine Tumor
- PMID: 33518610
- PMCID: PMC7925266
- DOI: 10.2169/internalmedicine.5208-20
Cardiac Metastasis Caused Fatal Ventricular Arrhythmia in a Patient with a Rectal Neuroendocrine Tumor
Abstract
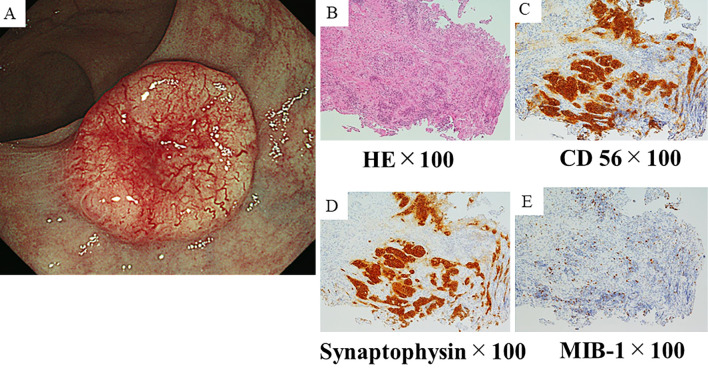
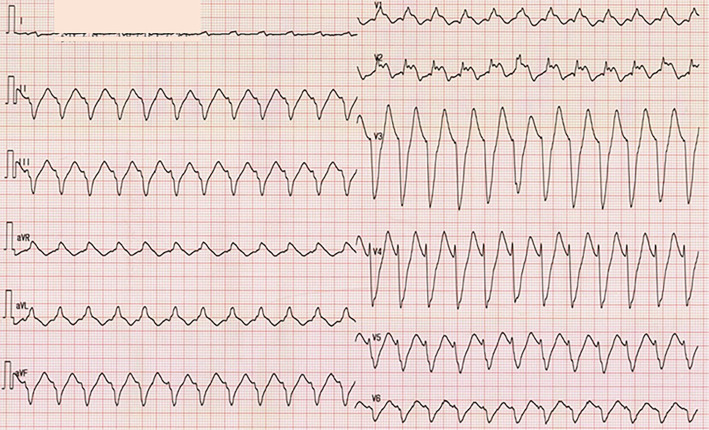
A 60-year-old man had received octreotide for a metastatic neuroendocrine tumor (NET) in the rectum. Computed tomography and ultrasonography revealed a cardiac tumor, diffuse thickness of the ventricular wall and pericardial effusion, which was diagnosed as cardiac metastasis. The metastatic lesions continued to grow despite the alteration of chemotherapy, and the patient complained of repeated syncope and was admitted to our hospital at 11 months after the diagnosis of cardiac metastasis. An electrocardiogram during syncope showed sustained ventricular tachycardia, which was considered to be caused by the cardiac metastasis. We herein report a case of NET with cardiac metastasis which caused lethal arrhythmia along with a review of the pertinent literature.
Keywords: cardiac metastasis; neuroendocrine tumor; ventricular arrhythmia.
Conflict of interest statement
Mikihiro Fujiya: Honoraria, Teijin Pharma and Nobelpharma; Research funding, Nobelpharma.
Figures



Similar articles
-
Rectal Neuroendocrine Tumor with Synchronous Pancreatic Metastasis: A Case Report.Tokai J Exp Clin Med. 2018 Jul 20;43(2):38-44. Tokai J Exp Clin Med. 2018. PMID: 29961930
-
Ventricular tachycardia associated with radiation-induced cardiac sarcoma.Tex Heart Inst J. 2014 Dec 1;41(6):620-5. doi: 10.14503/THIJ-13-3378. eCollection 2014 Dec. Tex Heart Inst J. 2014. PMID: 25593527 Free PMC article. Review.
-
Heart failure due to right ventricular metastatic neuroendocrine tumor.Int J Cardiol. 2008 May 23;126(2):e25-6. doi: 10.1016/j.ijcard.2007.01.007. Epub 2007 Mar 29. Int J Cardiol. 2008. PMID: 17395312
-
[Development of cardiac tamponade and emergence of arrhythmia during chemotherapy for diffuse large B-cell lymphoma].Rinsho Ketsueki. 2019;60(6):577-581. doi: 10.11406/rinketsu.60.577. Rinsho Ketsueki. 2019. PMID: 31281147 Japanese.
-
A primary neuroendocrine tumor of the left ventricle presenting with diarrhea-an unusual experience and literature review.Diagn Pathol. 2020 Apr 3;15(1):32. doi: 10.1186/s13000-020-00935-x. Diagn Pathol. 2020. PMID: 32245475 Free PMC article. Review.
Cited by
-
Radioligand therapy (RLT) used to treat cardiac metastasis of pancreatic neuroendocrine tumor.Clin Case Rep. 2024 Mar 5;12(3):e8622. doi: 10.1002/ccr3.8622. eCollection 2024 Mar. Clin Case Rep. 2024. PMID: 38449894 Free PMC article.
References
-
- Ito T, Igarashi H, Nakamura K, et al. . Epidemiological trends of pancreatic and gastrointestinal neuroendocrine tumors in Japan: a nationwide survey analysis. J Gastroenterol 50: 58-64, 2015. - PubMed
-
- Cives M, Strosberg JR. Gastroenteropancreatic neuroendocrine tumors. CA Cancer J Clin 68: 471-487, 2018. - PubMed
-
- Pavel M, Grossman A, Arnold R, et al. . ENETS consensus guidelines for the management of brain, cardiac and ovarian metastases from neuroendocrine tumors. Neuroendocrinology 91: 326-332, 2010. - PubMed
-
- Maréchaux S, Dagorn J, Gaxotte V, et al. . Myocardial metastasis of a bronchial carcinoid. Eur Heart J 28: 391, 2007. - PubMed
-
- Yeung HW, Imbriaco M, Zhang JJ, et al. . Visualization of myocardial metastasis of carcinoid tumor by indium-111-pentetreotide. J Nucl Med 37: 1528-1530, 1996. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical