

Atypical Resting-State Functional Connectivity Dynamics Correlate With Early Cognitive Dysfunction in HIV Infection
- PMID: 33519683
- PMCID: PMC7841016
- DOI: 10.3389/fneur.2020.606592
Atypical Resting-State Functional Connectivity Dynamics Correlate With Early Cognitive Dysfunction in HIV Infection
Abstract
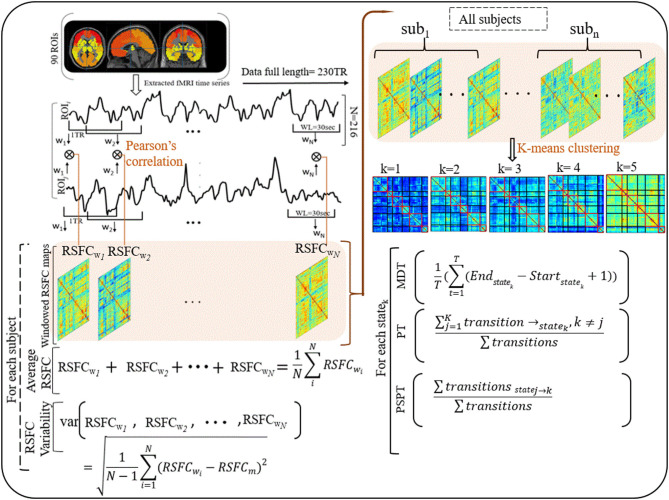
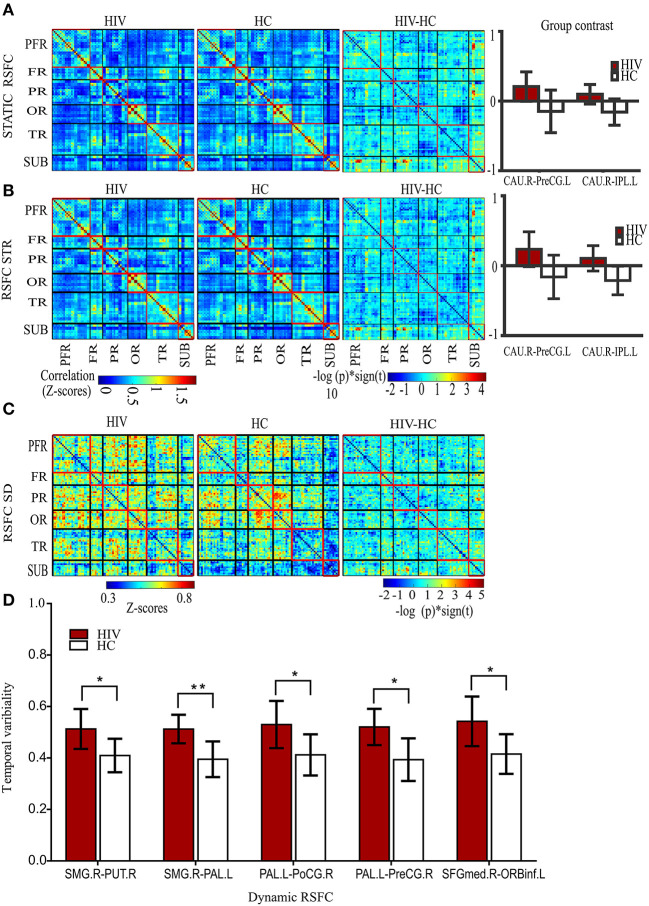
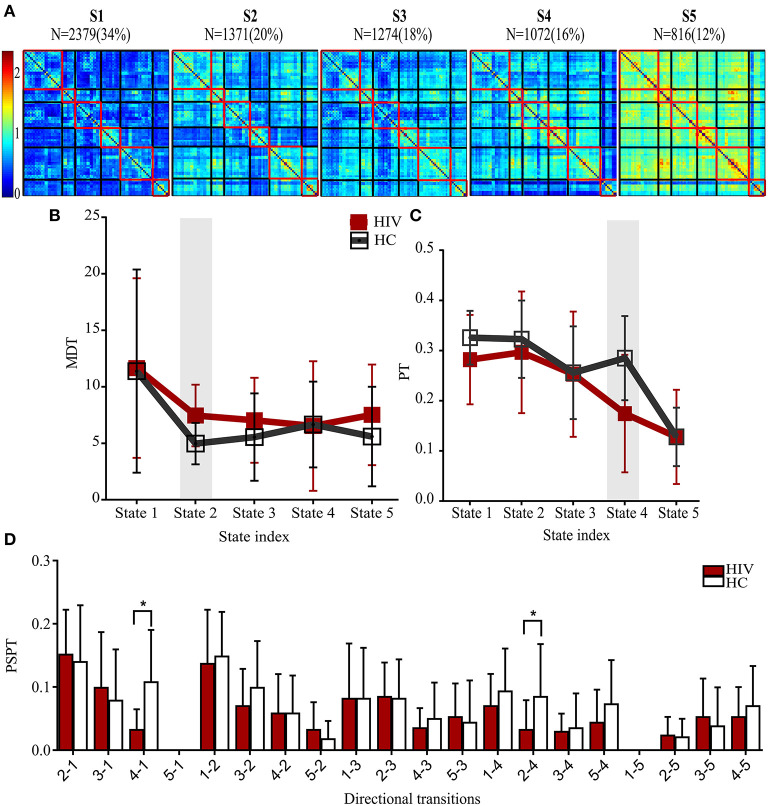
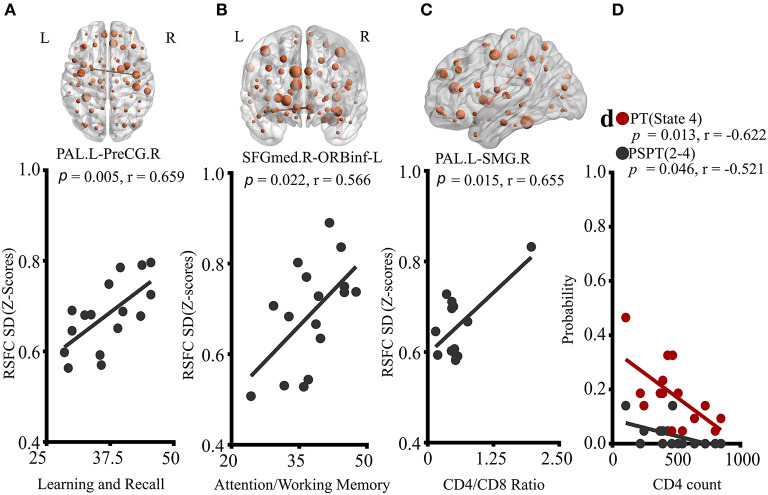
Purpose: Previous studies have shown that HIV affects striato-cortical regions, leading to persisting cognitive impairment in 30-70% of the infected individuals despite combination antiretroviral therapy. This study aimed to investigate brain functional dynamics whose deficits might link to early cognitive decline or immunologic deterioration. Methods: We applied sliding windows and K-means clustering to fMRI data (HIV patients with asymptomatic neurocognitive impairment and controls) to construct dynamic resting-state functional connectivity (RSFC) maps and identify states of their reoccurrences. The average and variability of dynamic RSFC, and the dwelling time and state transitioning of each state were evaluated. Results: HIV patients demonstrated greater variability in RSFC between the left pallidum and regions of right pre-central and post-central gyri, and between the right supramarginal gyrus and regions of the right putamen and left pallidum. Greater variability was also found in the frontal RSFC of pars orbitalis of the left inferior frontal gyrus and right superior frontal gyrus (medial). While deficits in learning and memory recall of HIV patients related to greater striato-sensorimotor variability, deficits in attention and working memory were associated with greater frontal variability. Greater striato-parietal variability presented a strong link with immunologic function (CD4+/CD8+ ratio). Furthermore, HIV-infected patients exhibited longer time and reduced transitioning in states typified by weaker connectivity in specific networks. CD4+T-cell counts of the HIV-patients were related to reduced state transitioning. Conclusion: Our findings suggest that HIV alters brain functional connectivity dynamics, which may underlie early cognitive impairment. These findings provide novel insights into our understanding of HIV pathology, complementing the existing knowledge.
Keywords: HIV-associated neurocognitive disorders; brain resting-state functional connectivity dynamics; fMRI; functional connectivity; temporal variability.
Copyright © 2021 Nguchu, Zhao, Wang, Li, Wei, Uwisengeyimana, Wang, Qiu and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous