

Dyslipidemia and cardiovascular disease risk factors in patients with type 1 diabetes: A single-center experience
- PMID: 33520108
- PMCID: PMC7807252
- DOI: 10.4239/wjd.v12.i1.56
Dyslipidemia and cardiovascular disease risk factors in patients with type 1 diabetes: A single-center experience
Abstract
Background: Type 1 diabetes (T1D) contributes to altered lipid profiles and increases the risk of cardiovascular disease (CVD). Youth with T1D may have additional CVD risk factors within the first decade of diagnosis.
Aim: To examine risk factors for dyslipidemia in young subjects with T1D.
Methods: Longitudinal and cross-sectional retrospective study of 170 young subjects with T1D (86 males; baseline mean age 12.2 ± 5.6 years and hemoglobin A1c 8.4% ± 1.4%) were followed in a single tertiary diabetes center for a median duration of 15 years. Predictors for outcomes of lipid profiles at last visit (total cholesterol [TC], triglycerides [TGs], low-density lipoprotein-cholesterol [LDL-c], and high-density lipoprotein-cholesterol [HDL-c]) were analyzed by stepwise linear regression models.
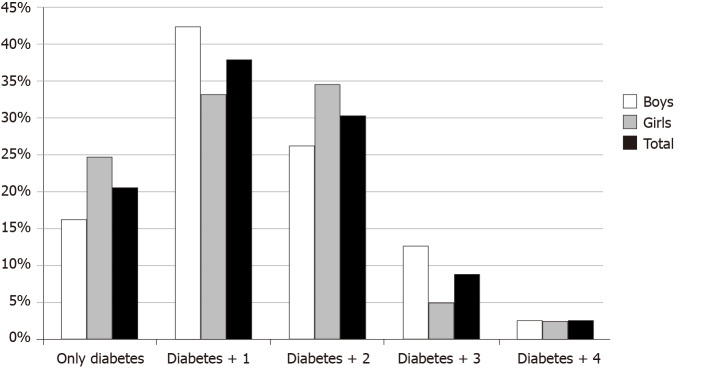
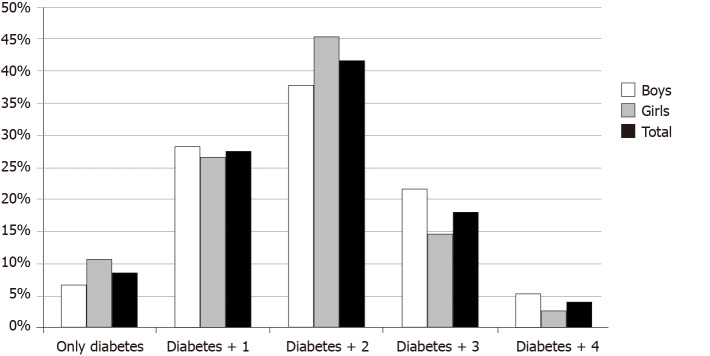
Results: At baseline, 79.5% of the patients had at least one additional CVD risk factor (borderline dyslipidemia/dyslipidemia [37.5%], pre-hypertension/hypertension [27.6%], and overweight/obesity [16.5%]) and 41.6% had multiple (≥ 2) CVD risk factors. A positive family history of at least one CVD risk factor in a first-degree relative was reported in 54.1% of the cohort. Predictors of elevated TC: family history of CVD (β[SE] = 23.1[8.3], P = 0.006); of elevated LDL-c: baseline diastolic blood pressure (DBP) (β[SE] = 11.4[4.7], P = 0.003) and family history of CVD (β[SE] = 20.7[6.8], P = 0.017); of elevated TGs: baseline DBP (β[SE] = 23.8[9.1], P = 0.010) and family history of CVD (β[SE] = 31.0[13.1], P = 0.020); and of low HDL-c levels: baseline DBP (β[SE] = 4.8[2.1], P = 0.022]).
Conclusion: Our findings suggest that elevated lipid profiles are associated with DBP and a positive family history of CVD. It is of utmost importance to prevent and control modifiable risk factors such as these, as early as childhood, given that inadequate glycemic control and elevation in blood pressure intensify the risk of dyslipidemia.
Keywords: Cardiovascular disease risk factors; Children and adolescents; Dyslipidemia; Family history of cardiovascular disease risk factors; Hypertension; Type 1 diabetes.
©The Author(s) 2021. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All authors confirm that no potential conflicts of interest relevant to this article were reported.
Figures
Similar articles
-
A longitudinal assessment of lipids in youth with type 1 diabetes.Pediatr Diabetes. 2011 Jun;12(4 Pt 2):365-71. doi: 10.1111/j.1399-5448.2010.00733.x. Epub 2011 Mar 11. Pediatr Diabetes. 2011. PMID: 21392191
-
Correlation between hemoglobin A1c and serum lipid profile in Afghani patients with type 2 diabetes: hemoglobin A1c prognosticates dyslipidemia.Ther Adv Endocrinol Metab. 2017 Apr;8(4):51-57. doi: 10.1177/2042018817692296. Epub 2017 Mar 20. Ther Adv Endocrinol Metab. 2017. PMID: 28507727 Free PMC article.
-
Overweight and obese youth with type 1 or type 2 diabetes share similar elevation in triglycerides during middle and late adolescence.Obes Res Clin Pract. 2022 Mar-Apr;16(2):138-143. doi: 10.1016/j.orcp.2022.03.003. Epub 2022 Apr 13. Obes Res Clin Pract. 2022. PMID: 35430167
-
Preventing Cardiovascular Complications in Type 1 Diabetes: The Need for a Lifetime Approach.Front Pediatr. 2021 Jun 9;9:696499. doi: 10.3389/fped.2021.696499. eCollection 2021. Front Pediatr. 2021. PMID: 34178905 Free PMC article. Review.
-
Sex-Related Differences in Cardiovascular Disease Risk Profile in Children and Adolescents with Type 1 Diabetes.Int J Mol Sci. 2021 Sep 22;22(19):10192. doi: 10.3390/ijms221910192. Int J Mol Sci. 2021. PMID: 34638531 Free PMC article. Review.
Cited by
-
Sex differences in body composition in youth with type 1 diabetes and its predictive value in cardiovascular disease risk assessment.Diabetes Metab Res Rev. 2023 Jan;39(1):e3584. doi: 10.1002/dmrr.3584. Epub 2022 Nov 5. Diabetes Metab Res Rev. 2023. PMID: 36269559 Free PMC article.
-
Knowledge and Performance of Iranian Internists Regarding Dyslipidemia According to Lipid Guidelines and Their Relationships with Personal and Occupational Characteristics.J Tehran Heart Cent. 2024 Jan;19(1):14-24. doi: 10.18502/jthc.v19i1.15532. J Tehran Heart Cent. 2024. PMID: 39712359 Free PMC article.
-
Impact of statin treatment on cardiovascular risk in patients with type 1 diabetes: a population-based cohort study.J Transl Med. 2023 Nov 12;21(1):806. doi: 10.1186/s12967-023-04691-6. J Transl Med. 2023. PMID: 37951886 Free PMC article.
-
Prevalence of autoimmune comorbidities and association with glycemic control by CGM-derived parameters in type 1 diabetes.Endocrine. 2025 Jul 15. doi: 10.1007/s12020-025-04354-0. Online ahead of print. Endocrine. 2025. PMID: 40663292
References
-
- Patterson CC, Harjutsalo V, Rosenbauer J, Neu A, Cinek O, Skrivarhaug T, Rami-Merhar B, Soltesz G, Svensson J, Parslow RC, Castell C, Schoenle EJ, Bingley PJ, Dahlquist G, Jarosz-Chobot PK, Marčiulionytė D, Roche EF, Rothe U, Bratina N, Ionescu-Tirgoviste C, Weets I, Kocova M, Cherubini V, Rojnic Putarek N, deBeaufort CE, Samardzic M, Green A. Trends and cyclical variation in the incidence of childhood type 1 diabetes in 26 European centres in the 25 year period 1989-2013: a multicentre prospective registration study. Diabetologia. 2019;62:408–417. - PubMed
-
- DIAMOND Project Group. Incidence and trends of childhood Type 1 diabetes worldwide 1990-1999. Diabet Med. 2006;23:857–866. - PubMed
-
- Mayer-Davis EJ, Lawrence JM, Dabelea D, Divers J, Isom S, Dolan L, Imperatore G, Linder B, Marcovina S, Pettitt DJ, Pihoker C, Saydah S, Wagenknecht L SEARCH for Diabetes in Youth Study. Incidence Trends of Type 1 and Type 2 Diabetes among Youths, 2002-2012. N Engl J Med. 2017;376:1419–1429. - PMC - PubMed
-
- Berenson GS, Wattigney WA, Tracy RE, Newman WP 3rd, Srinivasan SR, Webber LS, Dalferes ER Jr, Strong JP. Atherosclerosis of the aorta and coronary arteries and cardiovascular risk factors in persons aged 6 to 30 years and studied at necropsy (The Bogalusa Heart Study) Am J Cardiol. 1992;70:851–858. - PubMed
-
- Singh TP, Groehn H, Kazmers A. Vascular function and carotid intimal-medial thickness in children with insulin-dependent diabetes mellitus. J Am Coll Cardiol. 2003;41:661–665. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
