

A Safe Anti-A2 Titer for a Successful A2 Incompatible Kidney Transplantation: A Single-center Experience and Review of the Literature
- PMID: 33521251
- PMCID: PMC7837880
- DOI: 10.1097/TXD.0000000000001099
A Safe Anti-A2 Titer for a Successful A2 Incompatible Kidney Transplantation: A Single-center Experience and Review of the Literature
Abstract
Background: Kidney allocation system allows blood type B candidates accept kidneys from A2/A2B donors. There is no mandate by UNOS on which the anti-A2 level is acceptable. We aimed to investigate the safety of kidney transplant in blood group B patients with anti-A2 titers ≤16.
Methods: We performed 41 A2-incompatible kidney transplants in blood group B recipients between May 2015 and September 2019. Clinical outcomes were compared with a control group of 75 blood group B recipients who received blood group compatible kidney transplantation at the same period.
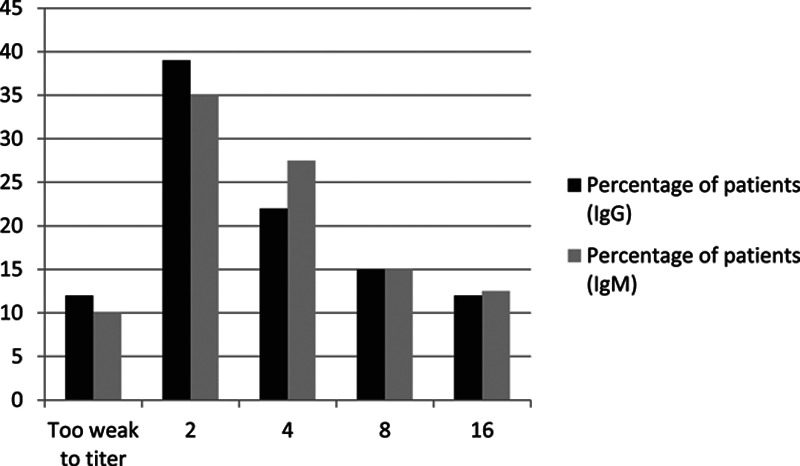
Results: Of the 41 recipients, 85% were male, 48% African American, with a median age of 53 (20-73) y. Thirty-eight (93%) were deceased-donor and 3 (7%) were living-donor kidney transplant recipients. Pretransplant anti-A2 IgG titers were 2 in 16, 4 in 9, 8 in 6, and 16 in 5 and too weak to titer in 5 recipients. Eight patients had pretransplant donor-specific antibodies. During a median follow-up of 32.6 mo (6-57.3) patient and graft survival were 100% and 92% in the A2-incompatible kidney transplant group, and 91% and 92% in the blood group compatible group, respectively. Twelve A2-incompatible recipients underwent a 21 clinically indicated kidney biopsies at a median 28 d (6-390) after transplantation. None of the patients developed acute antibody-mediated rejection and 2 patients (5%) had acute T-cell-mediated rejection. Interestingly, peritubular capillary C4d positivity was seen in 7 biopsies which did not have any findings of acute rejection or microvascular inflammation but not in any of the rejection-free biopsies in the control group. C4d positivity was persistent in 5 of those patients who had follow-up biopsies.
Conclusions: A2-incompatible transplantation is safe in patients with anti-A2 titers ≤16 with excellent short-term kidney allograft outcomes. C4d positivity is frequent in allograft biopsies without acute rejection.
Copyright © 2021 The Author(s). Transplantation Direct. Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no funding or conflicts of interest.
Figures
Similar articles
-
A2/A2B Deceased Donor Kidney Transplantation Using A2 Titers Improves Access to Kidney Transplantation: A Single-Center Study.Kidney Med. 2024 May 21;6(7):100843. doi: 10.1016/j.xkme.2024.100843. eCollection 2024 Jul. Kidney Med. 2024. PMID: 38947773 Free PMC article.
-
A2/A2B to B kidney transplantation outcomes: A single center 7-year experience.Clin Transplant. 2024 Apr;38(4):e15295. doi: 10.1111/ctr.15295. Clin Transplant. 2024. PMID: 38545909
-
Transplantation of ABO A2 kidneys into O recipients: do IgM anti-A1 titers matter?Clin Transplant. 2015 Apr;29(4):379-82. doi: 10.1111/ctr.12527. Epub 2015 Feb 26. Clin Transplant. 2015. PMID: 25659826 Clinical Trial.
-
Organ Preservation Solutions in Transplantation: A Literature Review.Exp Clin Transplant. 2021 Jun;19(6):511-521. doi: 10.6002/ect.2020.0506. Epub 2021 Mar 31. Exp Clin Transplant. 2021. PMID: 33797354 Review.
-
ABO incompatible kidney transplantation.Curr Opin Nephrol Hypertens. 2007 Nov;16(6):529-34. doi: 10.1097/MNH.0b013e3282f02218. Curr Opin Nephrol Hypertens. 2007. PMID: 18089966 Review.
Cited by
-
A2/A2B Deceased Donor Kidney Transplantation Using A2 Titers Improves Access to Kidney Transplantation: A Single-Center Study.Kidney Med. 2024 May 21;6(7):100843. doi: 10.1016/j.xkme.2024.100843. eCollection 2024 Jul. Kidney Med. 2024. PMID: 38947773 Free PMC article.
-
Outcomes of A2/A2B to B Deceased Donor Kidney Transplantation: A Retrospective Study.Cureus. 2024 Nov 10;16(11):e73368. doi: 10.7759/cureus.73368. eCollection 2024 Nov. Cureus. 2024. PMID: 39659322 Free PMC article.
References
-
- Scurt FG, Ewert L, Mertens PR, et al. Clinical outcomes after ABO-incompatible renal transplantation: a systematic review and meta-analysis. Lancet. 2019; 393:2059–2072 - PubMed
-
- Bryan CF, Cherikh WS, Sesok-Pizzini DA. A2 /A2 B to B renal transplantation: past, present, and future directions. Am J Transplant. 2016; 16:11–20 - PubMed
-
- Breimer ME, Mölne J, Nordén G, et al. Blood group A and B antigen expression in human kidneys correlated to A1/A2/B, Lewis, and secretor status. Transplantation. 2006; 82:479–485 - PubMed
-
- Williams WW, Cherikh WS, Young CJ, et al. First report on the OPTN national variance: allocation of A2 /A2 B deceased donor kidneys to blood group B increases minority transplantation. Am J Transplant. 2015; 15:3134–3142 - PubMed
-
- Bryan CF, Winklhofer FT, Murillo D, et al. Improving access to kidney transplantation without decreasing graft survival: long-term outcomes of blood group A2/A2B deceased donor kidneys in B recipients. Transplantation. 2005; 80:75–80 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
