

Delays in ST-Elevation Myocardial Infarction Care During the COVID-19 Lockdown: An Observational Study
- PMID: 33521615
- PMCID: PMC7834324
- DOI: 10.1016/j.cjco.2020.12.009
Delays in ST-Elevation Myocardial Infarction Care During the COVID-19 Lockdown: An Observational Study
Abstract
Background: Management of ST-elevated myocardial infarction (STEMI) necessitates rapid reperfusion. Delays prolong myocardial ischemia and increase the risk of complications, including death. The COVID-19 pandemic may have impacted STEMI management. We evaluated the relative volume of hospitalizations and clinical time intervals within a regional STEMI system.
Methods: 494 patients with STEMI were grouped into pre-lockdown, lockdown and re-opening cohorts. Clinical, temporal and outcome data were collected and compared between groups for both urban and rural patients, receiving primary percutaneous coronary intervention (PCI) and pharmacoinvasive revascularization, respectively. Data was compared to a 10-year historical comparator.
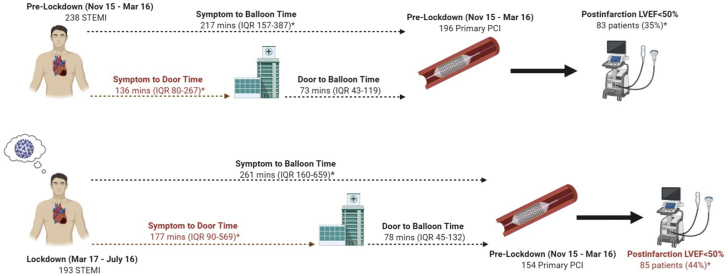
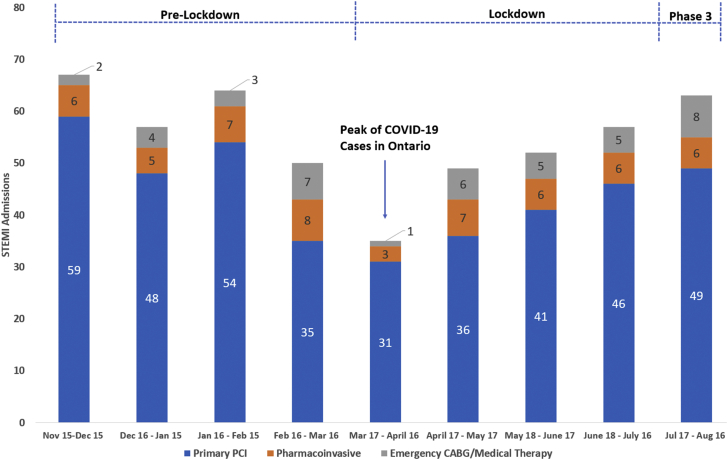
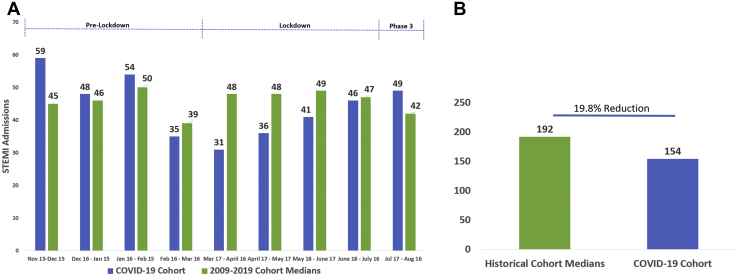
Results: During pre-lockdown there was 238 cases versus 193 in lockdown; a 19.0% reduction in volume. When lockdown was compared to the median caseload from a 10-year historical cohort, a 19.8% reduction was observed. For patients treated with primary PCI during lockdown, median symptom-to-balloon time increased by 44-minutes [217 (IQR 157-387) vs. 261 (160-659) minutes; p=0.03]; driven by an increase in median symptom-to-door time of 41-minutes [136 (IQR 80-267) vs. 177 (IQR 90-569) minutes; p<0.01]. Only patients transferred from non-PCI facilities demonstrated an increase in door-to-reperfusion time [116 (IQR 93-150) vs. 139 (IQR 100-199) minutes; p<0.01]. More patients had left ventricular dysfunction during the lockdown [35% vs. 44%; p=0.04], but there was no difference in mortality.
Conclusion: During the COVID-19 lockdown, fewer patients presented with STEMI. Time-to-reperfusion was significantly prolonged and appeared driven predominantly by patient-level and transfer delays. Public education and systems-level changes will be integral to STEMI care during the second wave of COVID-19.
Contexte: La prise en charge de l’infarctus du myocarde avec élévation du segment ST (STEMI) nécessite une reperfusion rapide. Tout retard de reperfusion prolonge l’ischémie myocardique et augmente le risque de complications, y compris le risque de décès. Il est possible que la pandémie de COVID-19 ait nui à la prise en charge du STEMI. Nous avons donc évalué le nombre relatif d’hospitalisations et le temps écoulé avant la reperfusion au sein d’un système régional de traitement des STEMI.
Méthodologie: Au total, 494 patients ayant présenté un STEMI ont été divisés en trois cohortes : préconfinement, confinement et déconfinement. Les données cliniques et temporelles et les données relatives aux résultats ont été recueillies et comparées entre les groupes pour les patients vivant en milieu urbain et en milieu rural, les patients ayant subi une intervention coronarienne percutanée (ICP) en soins primaires et les patients ayant subi une revascularisation pharmaco-effractive, respectivement. Les résultats ont été comparés aux données historiques des dix dernières années.
Résultats: On a dénombré 238 cas durant la période précédant le confinement comparativement à 193 durant le confinement, ce qui représente une diminution de 19,0 %. Si on compare les données de la période de confinement à celles de la cohorte historique des 10 dernières années, on observe une réduction de 19,8 % du nombre médian de cas survenus. Dans le cas des patients traités par ICP en soins primaires durant le confinement, le temps médian écoulé entre l’apparition des symptômes et l’insertion du ballonnet a augmenté de 44 minutes (217 [intervalle interquartile {IIQ} : 157 à 387], par rapport à 261 [IIQ : 160 à 659] minutes; p = 0,03), en raison d’une augmentation de 41 minutes (136 [IIQ : 80 à 267] vs 177 [IIQ : 90 à 569] minutes; p < 0,01) du temps médian écoulé entre l’apparition des symptômes et l’arrivée à l’hôpital. Seuls les patients transférés depuis un établissement n’ayant pas les moyens d’effectuer une ICP ont affiché une augmentation du temps écoulé entre l’arrivée à l’hôpital et la reperfusion (116 [IIQ : 93 à 150] vs 139 [IIQ : 100 à 199] minutes; p < 0,01). Un plus grand nombre de patients ont présenté une dysfonction ventriculaire gauche durant le confinement (35 % vs 44 %; p = 0,04), mais il n’y avait pas de différence quant à la mortalité.
Conclusions: Pendant le confinement dû à la COVID-19, le nombre de patients hospitalisés pour un STEMI a diminué. Le temps écoulé avant la reperfusion était significativement plus long; cette augmentation semble principalement attribuable au temps écoulé entre l’apparition des symptômes et l’arrivée à l’hôpital et à la nécessité de transférer les patients vers un établissement en mesure d’effectuer une ICP. La sensibilisation du public et des modifications à l’échelle des systèmes devront faire partie de la stratégie de traitement du STEMI pendant la deuxième vague de la pandémie de COVID-19.
© 2020 Published by Elsevier Inc. on behalf of the Canadian Cardiovascular Society.
Figures
References
-
- Daily COVID-19 Dashboard–Ottawa Public Health. https://www.ottawapublichealth.ca/en/reports-research-and-statistics/dai... Available at:
-
- COVID-19 Guidance for the Health Sector–Ministry Programs–Health Care Professionals –MOH. http://www.health.gov.on.ca/en/pro/programs/publichealth/coronavirus/201... Available at:
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
