

Cell-free DNA tissues of origin by methylation profiling reveals significant cell, tissue, and organ-specific injury related to COVID-19 severity
- PMID: 33521749
- PMCID: PMC7836424
- DOI: 10.1016/j.medj.2021.01.001
Cell-free DNA tissues of origin by methylation profiling reveals significant cell, tissue, and organ-specific injury related to COVID-19 severity
Abstract
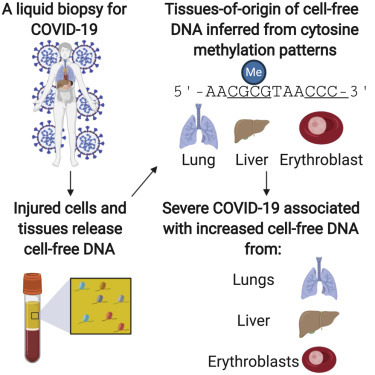
Background: Coronavirus disease 2019 (COVID-19) primarily affects the lungs, but evidence of systemic disease with multi-organ involvement is emerging. Here, we developed a blood test to broadly quantify cell-, tissue-, and organ-specific injury due to COVID-19.
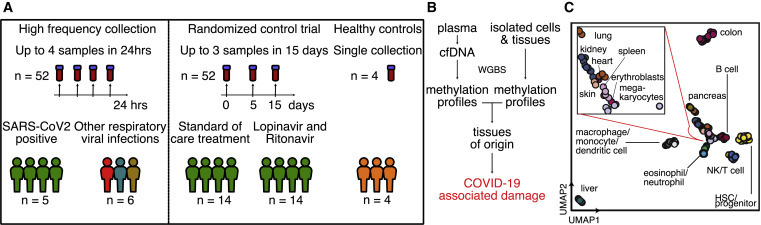
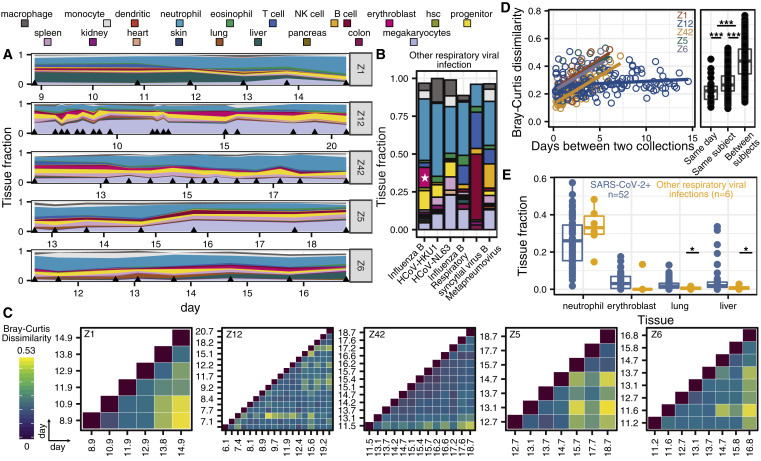
Methods: Our test leverages genome-wide methylation profiling of circulating cell-free DNA in plasma. We assessed the utility of this test to identify subjects with severe disease in two independent, longitudinal cohorts of hospitalized patients. Cell-free DNA profiling was performed on 104 plasma samples from 33 COVID-19 patients and compared to samples from patients with other viral infections and healthy controls.
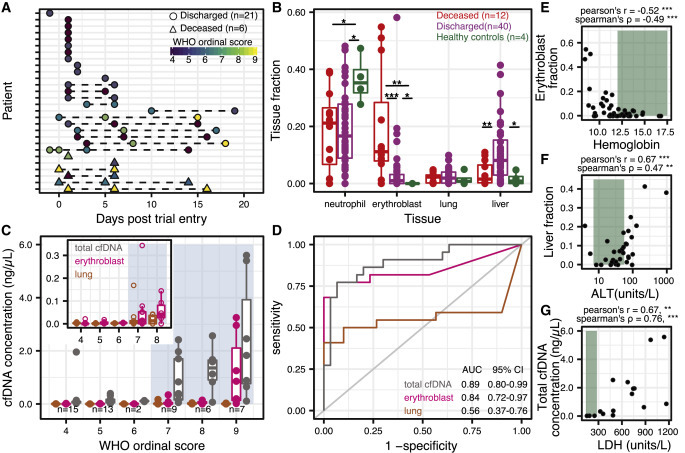
Findings: We found evidence of injury to the lung and liver and involvement of red blood cell progenitors associated with severe COVID-19. The concentration of cell-free DNA correlated with the World Health Organization (WHO) ordinal scale for disease progression and was significantly increased in patients requiring intubation.
Conclusions: This study points to the utility of cell-free DNA as an analyte to monitor and study COVID-19.
Funding: This work was supported by NIH grants 1DP2AI138242 (to I.D.V.), R01AI146165 (to I.D.V., M.P.C., F.M.M., and J.R.), 1R01AI151059 (to I.D.V.), K08-CA230156 (to W.G.), and R33-AI129455 to C.Y.C., a Synergy award from the Rainin Foundation (to I.D.V.), a SARS-CoV-2 seed grant at Cornell (to I.D.V.), a National Sciences and Engineering Research Council of Canada fellowship PGS-D3 (to A.P.C.), and a Burroughs-Wellcome CAMS Award (to W.G.). D.C.V. is supported by a Fonds de la Recherche en Sante du Quebec Clinical Research Scholar Junior 2 award. C.Y.C. is supported by the California Initiative to Advance Precision Medicine, and the Charles and Helen Schwab Foundation.
Keywords: COVID-19; SARS-CoV-2; cell-free DNA; disease severity; liquid biopsy; methylation; tissue injury.
© 2021 Elsevier Inc.
Conflict of interest statement
A.P.C., M.P.C., W.G., C.Y.C., D.C.V., and I.D.V. are inventors on a patent application submitted by Cornell University Center for Technology Licensing.
Figures
Update of
-
Cell-Free DNA in Blood Reveals Significant Cell, Tissue and Organ Specific injury and Predicts COVID-19 Severity.medRxiv [Preprint]. 2020 Jul 29:2020.07.27.20163188. doi: 10.1101/2020.07.27.20163188. medRxiv. 2020. Update in: Med. 2021 Apr 09;2(4):411-422.e5. doi: 10.1016/j.medj.2021.01.001. PMID: 32766608 Free PMC article. Updated. Preprint.
References
-
- Julien P., Julien G., Morgan C., et al. Pulmonary Embolism in COVID-19 Patients: Awareness of an Increased Prevalence. Circulation. 2020;142:184–186. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
