

Mortality risk prediction in elderly patients with cardiogenic shock: results from the CardShock study
- PMID: 33522124
- PMCID: PMC8006692
- DOI: 10.1002/ehf2.13224
Mortality risk prediction in elderly patients with cardiogenic shock: results from the CardShock study
Abstract
Aims: This study aimed to assess the utility of contemporary clinical risk scores and explore the ability of two biomarkers [growth differentiation factor-15 (GDF-15) and soluble ST2 (sST2)] to improve risk prediction in elderly patients with cardiogenic shock.
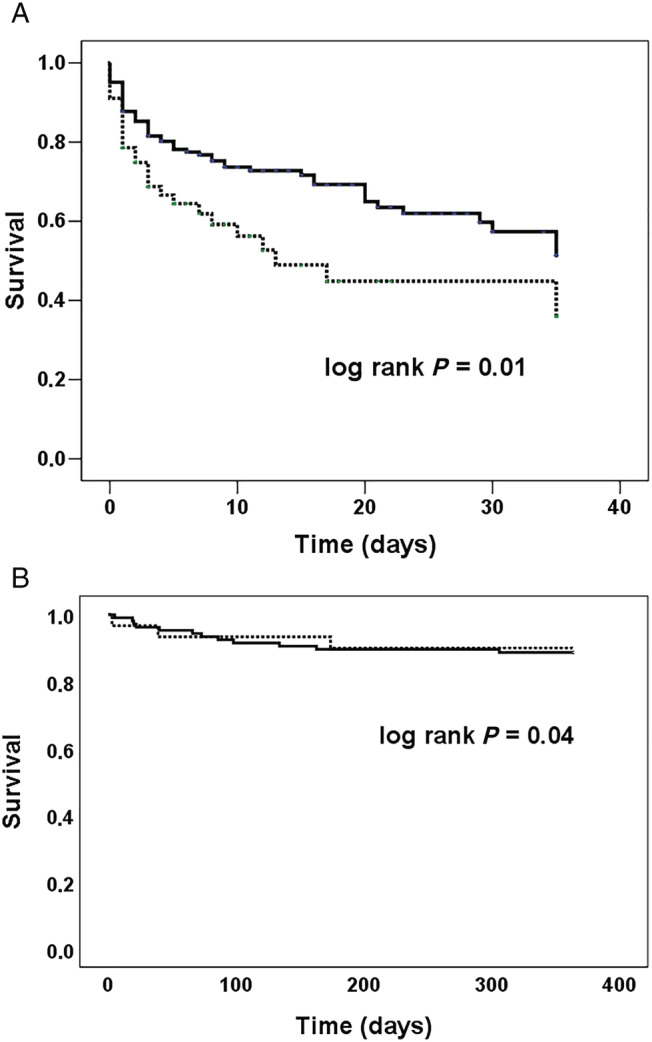
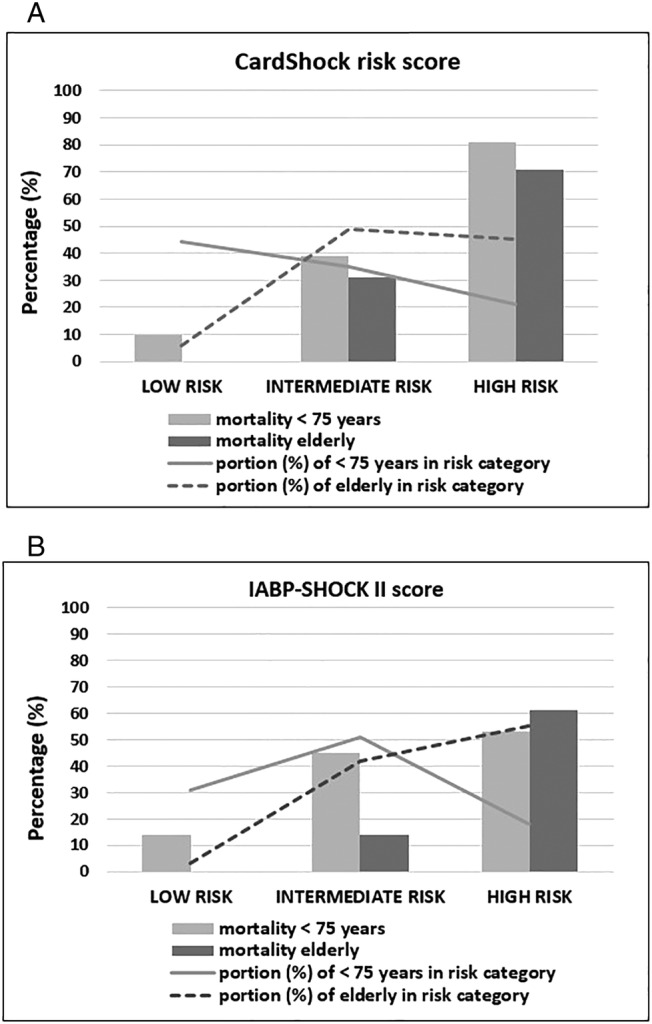
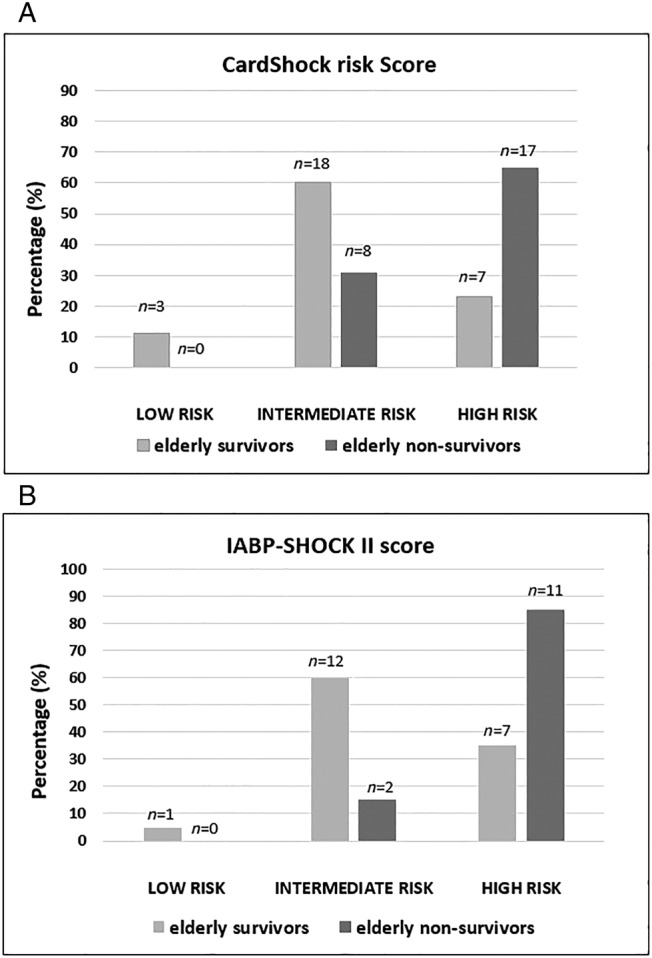
Methods and results: Patients (n = 219) from the multicentre CardShock study were grouped according to age (elderly ≥75 years and younger). Characteristics, management, and outcome between the groups were compared. The ability of the CardShock risk score and the IABP-SHOCK II score to predict in-hospital mortality and the additional value of GDF-15 and sST2 to improve risk prediction in the elderly was evaluated. The elderly constituted 26% of the patients (n = 56), with a higher proportion of women (41% vs. 21%, P < 0.05) and more co-morbidities compared with the younger. The primary aetiology of shock in the elderly was acute coronary syndrome (84%), with high rates of percutaneous coronary intervention (87%). Compared with the younger, the elderly had higher in-hospital mortality (46% vs. 33%; P = 0.08), but 1 year post-discharge survival was excellent in both age groups (90% in the elderly vs. 88% in the younger). In the elderly, the risk prediction models demonstrated an area under the curve of 0.75 for the CardShock risk score and 0.71 for the IABP-SHOCK II score. Incorporating GDF-15 and sST2 improved discrimination for both risk scores with areas under the curve ranging from 0.78 to 0.84.
Conclusions: Elderly patients with cardiogenic shock have higher in-hospital mortality compared with the younger, but post-discharge outcomes are similar. Contemporary risk scores proved useful for early mortality risk prediction also in the elderly, and risk stratification could be further improved with biomarkers such as GDF-15 or sST2.
Keywords: Biomarker; Cardiogenic shock; Elderly; GDF-15; Risk prediction; sST2.
© 2021 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
J.L. has received fees for lectures and advisory board meetings from Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Novartis, Pfizer, Roche Diagnostics, and Vifor Pharma. J.P. received honoraria for advisory meetings and lectures from Orion Pharma and Roche Diagnostics. V.C. received consulting honoraria from CVie Therapeutics Limited, Servier, and Windtree Therapeutics. All other authors have no conflicts to declare.
Figures
References
-
- Harjola VP, Lassus J, Sionis A, Køber L, Tarvasmäki T, Spinar J, Parissis J, Banaszewski M, Silva‐Cardoso J, Carubelli V, Di Somma S, Tolppanen H, Zeymer U, Thiele H, Nieminen MS, Mebazaa A. Clinical picture and risk prediction of short‐term mortality in cardiogenic shock. Eur J Heart Fail 2015; 17: 501–509. - PubMed
-
- Aissaoui N, Puymirat E, Juilliere Y, Jourdain P, Blanchard D, Schiele F, Guéret P, Popovic B, Ferrieres J, Simon T, Danchin N. Fifteen‐year trends in the management of cardiogenic shock and associated 1‐year mortality in elderly patients with acute myocardial infarction: the FAST‐MI programme. Eur J Heart Fail 2016; 18: 1144–1152. - PubMed
-
- Poss J, Koster J, Fuernau G, Eitel I, de Waha S, Ouarrak T, Lassus J, Harjola VP, Zeymer U, Thiele H, Desch S. Risk stratification for patients in cardiogenic shock after acute myocardial infarction. J Am Coll Cardiol 2017; 69: 1913–1920. - PubMed
-
- Miller RJH, Southern D, Wilton SB, James MT, Har B, Schnell G, van Diepen S, Grant ADM. Comparative prognostic accuracy of risk prediction models for cardiogenic shock. J Intensive Care Med 2019; 14: 885066619878125. - PubMed
-
- Hijazi Z, Oldgren J, Lindback J, Alexander JH, Connolly SJ, Eikelboom JW, Ezekowitz MD, Held C, Hylek EM, Lopes RD, Siegbahn A, Yusuf S, Granger CB, Wallentin L. A biomarker‐based risk score to predict death in patients with atrial fibrillation: the ABC (age, biomarkers, clinical history) death risk score. Eur Heart J 2018; 39: 477–485. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
