

Anterior Controllable Antedisplacement and Fusion (ACAF) vs Posterior Laminoplasty for Multilevel Severe Cervical Ossification of the Posterior Longitudinal Ligament: Retrospective Study Based on a Two-Year Follow-up
- PMID: 33522136
- PMCID: PMC7957409
- DOI: 10.1111/os.12856
Anterior Controllable Antedisplacement and Fusion (ACAF) vs Posterior Laminoplasty for Multilevel Severe Cervical Ossification of the Posterior Longitudinal Ligament: Retrospective Study Based on a Two-Year Follow-up
Abstract
Objectives: To compare the clinical outcomes of anterior controllable antedisplacement fusion (ACAF), a new surgical technique, with laminoplasty for the treatment of multilevel severe cervical ossification of the posterior longitudinal ligament (OPLL) based on a 2-year follow-up.
Methods: Clinical data of 53 patients (21 by ACAF and 32 by laminoplasty) who have accepted surgery for treatment of cervical myelopathy caused by multilevel severe OPLL (occupying rate ≥ 50%) from March 2015 to March 2017 were retrospectively reviewed and compared between ACAF group and laminoplasty group. Operative time, blood loss, and complications of the two groups were recorded. Radiographic parameters were evaluated pre- and postoperatively: cervical lordosis on X-ray, space available for the cord (SAC) and the occupying ratio (OR) on computed tomography (CT), and the anteroposterior (AP) diameter of the spinal cord at the narrowest level and the spinal cord curvature on magnetic resonance imaging (MRI). Japanese Orthopaedic Association (JOA) scoring was used to evaluate neurologic recovery. Statistical analysis was conducted to analyze the differences between two groups. The Mann-Whitney U test and chi square test were used to compare categorical variables. unpaired t test was used to compare continuous data.
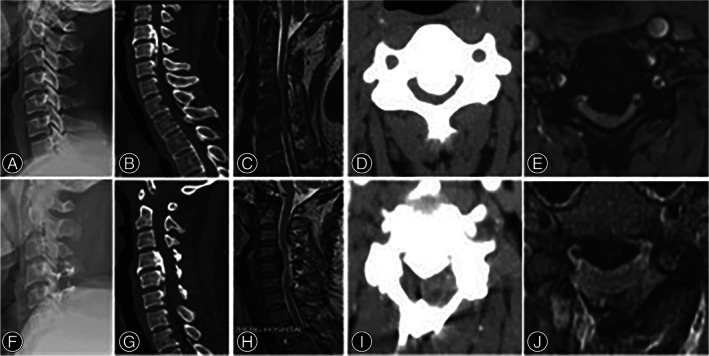
Results: All patients were followed up for at least 24 months. The operative time was longer in ACAF group (286.5 vs 178.2 min, P < 0.05). The blood loss showed no significant difference (291.6 vs 318.3 mL, P > 0.05). Less complications were observed in ACAF group than in laminoplasty group (one case [4.7%] of C5 palsy and one case [4.7%] of cerebrospinal fluid [CSF] leakage in ACAF group; four cases [12.5%] of C5 palsy, two cases [6.3%] of CSF leakage, and four cases [12.5%] of axial symptoms in laminoplasty group). The mean JOA score at last follow-up (14.6 vs 12.8, P < 0.05) and the improvement rate (IR) (63.8% vs 47.8%, P < 0.05) in ACAF group were superior to those in laminoplasty group significantly. The postoperative OR (16.7% vs 40.9%, P < 0.05), SAC (150.8 vs 110.5 mm2 , P < 0.05), AP spinal cord diameter (5.5 vs 4.2 mm, P < 0.05), and cervical lordosis (12.7° vs 4.7°, P < 0.05) were improved more considerably in ACAF group, with significant differences between two groups. Notably, the spinal cord on MRI showed a better curvature in ACAF group.
Conclusions: This study showed that ACAF is considered superior to laminoplasty for the treatment of multilevel severe OPLL as anterior direct decompression and better curvature of the spinal cord led to satisfactory neurologic outcomes and low complication rate.
Keywords: Anterior controllable antedisplacement and fusion (ACAF); Complication; Laminoplasty; Myelopathy; Ossification of the posterior longitudinal ligament (OPLL).
© 2021 The Authors. Orthopaedic Surgery published by Chinese Orthopaedic Association and John Wiley & Sons Australia, Ltd.
Figures





References
-
- Edwards CC, Heller JG, Murakami H. Corpectomy versus Laminoplasty for multilevel cervical myelopathy. Spine (Phila Pa 1976), 2002, 27: 1168–1175. - PubMed
-
- Fujimori T, Iwasaki M, Okuda S, et al. Long‐term results of cervical myelopathy due to ossification of the posterior longitudinal ligament with an occupying ratio of 60% or more. Spine (Phila Pa 1976), 2014, 39: 58–67. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
