

Association between perioperative fluid administration and postoperative outcomes: a 20-year systematic review and a meta-analysis of randomized goal-directed trials in major visceral/noncardiac surgery
- PMID: 33522953
- PMCID: PMC7849093
- DOI: 10.1186/s13054-021-03464-1
Association between perioperative fluid administration and postoperative outcomes: a 20-year systematic review and a meta-analysis of randomized goal-directed trials in major visceral/noncardiac surgery
Abstract
Background: Appropriate perioperative fluid management is of pivotal importance to reduce postoperative complications, which impact on early and long-term patient outcome. The so-called perioperative goal-directed therapy (GDT) approach aims at customizing perioperative fluid management on the individual patients' hemodynamic response. Whether or not the overall amount of perioperative volume infused in the context of GDT could influence postoperative surgical outcomes is unclear.
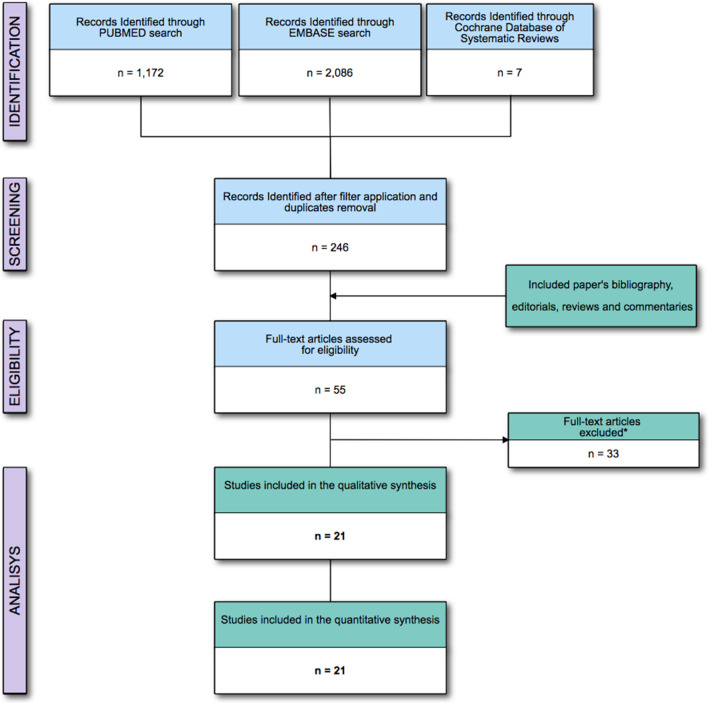
Methods: We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) comparing the efficacy of GDT approach between study population and control group in reducing postoperative complications and perioperative mortality, using MEDLINE, EMBASE and the Cochrane Controlled Clinical trials register. The enrolled studies were grouped considering the amount infused intraoperatively and during the first 24 h after the admission in the critical care unit (perioperative fluid).
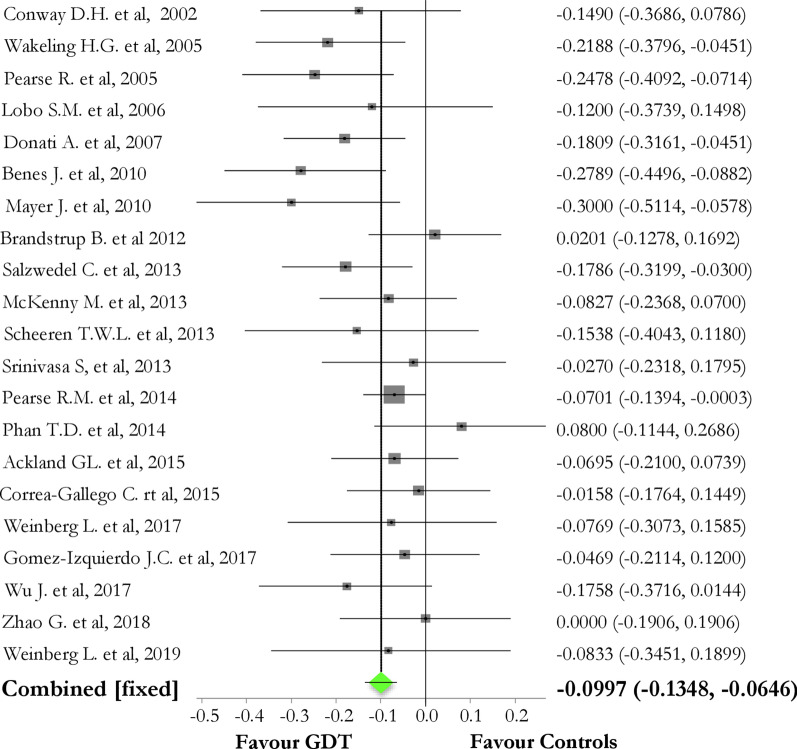
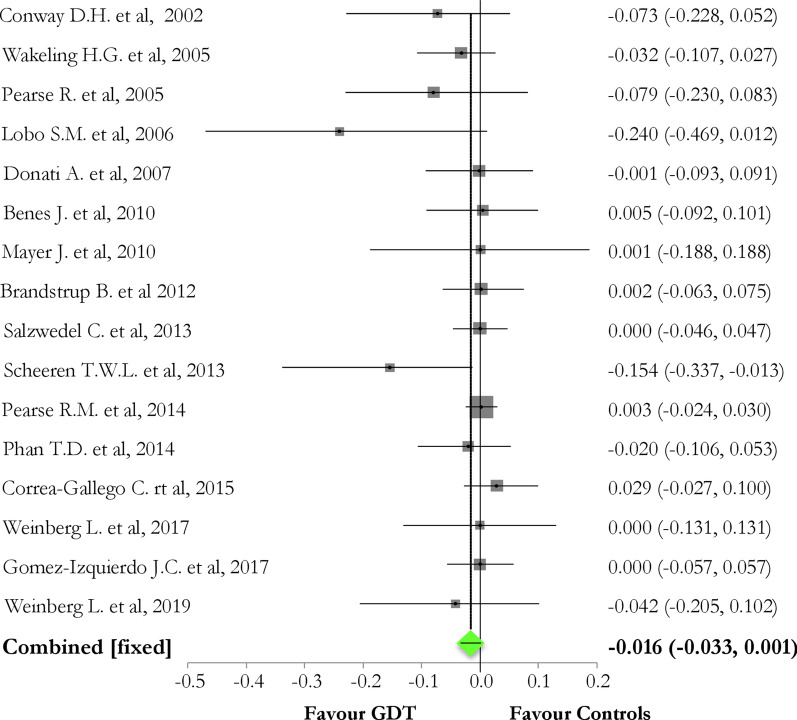
Results: The metanalysis included 21 RCTs enrolling 2729 patients with a median amount of perioperative fluid infusion of 4500 ml. In the studies reporting an overall amount below or above this threshold, the differences in postoperative complications were not statically significant between controls and GDT subgroup [43.4% vs. 34.2%, p value = 0.23 and 54.8% vs. 39.8%; p value = 0.09, respectively]. Overall, GDT reduced the overall rate of postoperative complications, as compared to controls [pooled risk difference (95% CI) = - 0.10 (- 0.14, - 0.07); Chi2 = 30.97; p value < 0.0001], but not to a reduction of perioperative mortality [pooled risk difference (95%CI) = - 0.016 (- 0.0334; 0.0014); p value = 0.07]. Considering the rate of organ-related postoperative events, GDT did not reduce neither renal (p value = 0.52) nor cardiovascular (p value = 0.86) or pulmonary (p value = 0.14) or neurological (p value = 0.44) or infective (p value = 0.12) complications.
Conclusions: Irrespectively to the amount of perioperative fluid administered, GDT strategy reduces postoperative complications, but not perioperative mortality.
Trial registration: CRD42020168866; Registration: February 2020 https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=168866.
Keywords: Fluids; Metanalysis; Perioperative goal-directed therapy; Postoperative complications; Surgery; Systematic review.
Conflict of interest statement
Dr. Messina received travel expenses and registration for meetings, congresses, and courses and lecture fees from Vygon; Prof. Cecconi is a consultant for Edwards Lifesciences, LiDCO and Cheetah Medical.
Figures
Comment in
-
Goal-directed therapy in the perioperative management: is a complete hemodynamics bundle of care better?Crit Care. 2021 Mar 16;25(1):105. doi: 10.1186/s13054-021-03527-3. Crit Care. 2021. PMID: 33726792 Free PMC article. No abstract available.
References
-
- Thompson JS, Baxter BT, Allison JG, Johnson FE, Lee KK, Park WY. Temporal patterns of postoperative complications. Arch Surg. 2003;138:596–602; discussion 602–593. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
