

Capture and visualization of live Mycobacterium tuberculosis bacilli from tuberculosis patient bioaerosols
- PMID: 33524021
- PMCID: PMC7877778
- DOI: 10.1371/journal.ppat.1009262
Capture and visualization of live Mycobacterium tuberculosis bacilli from tuberculosis patient bioaerosols
Abstract
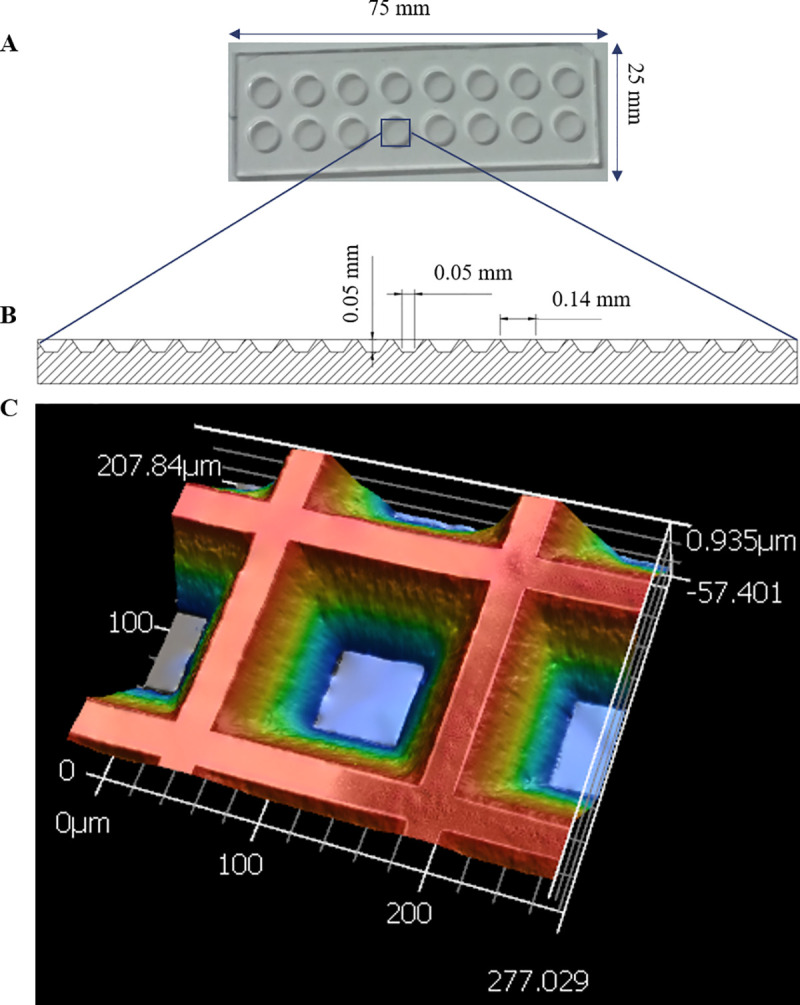
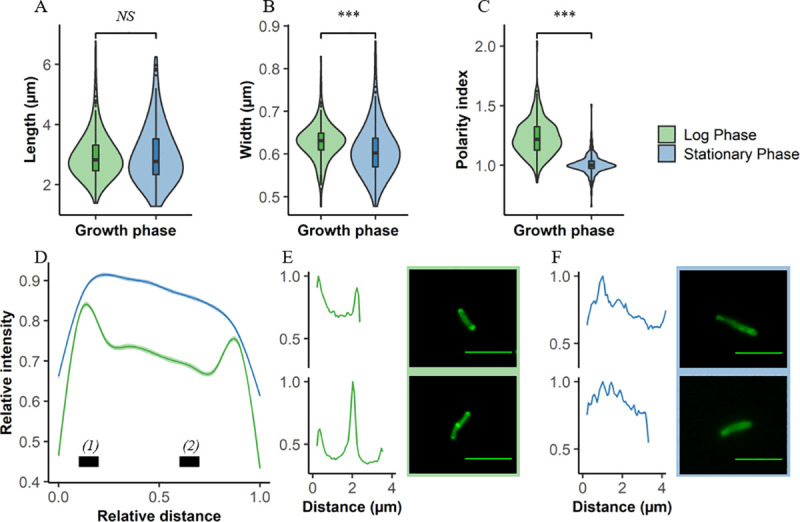
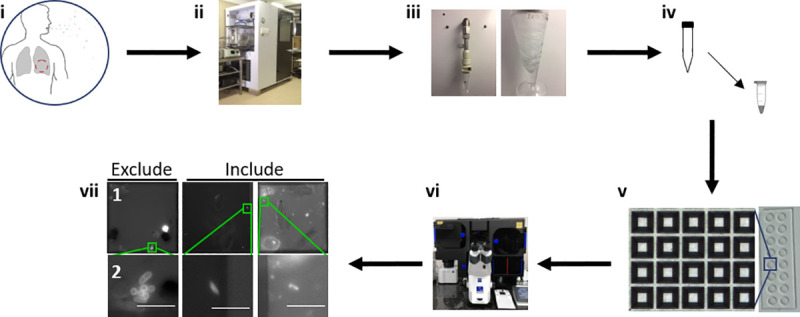
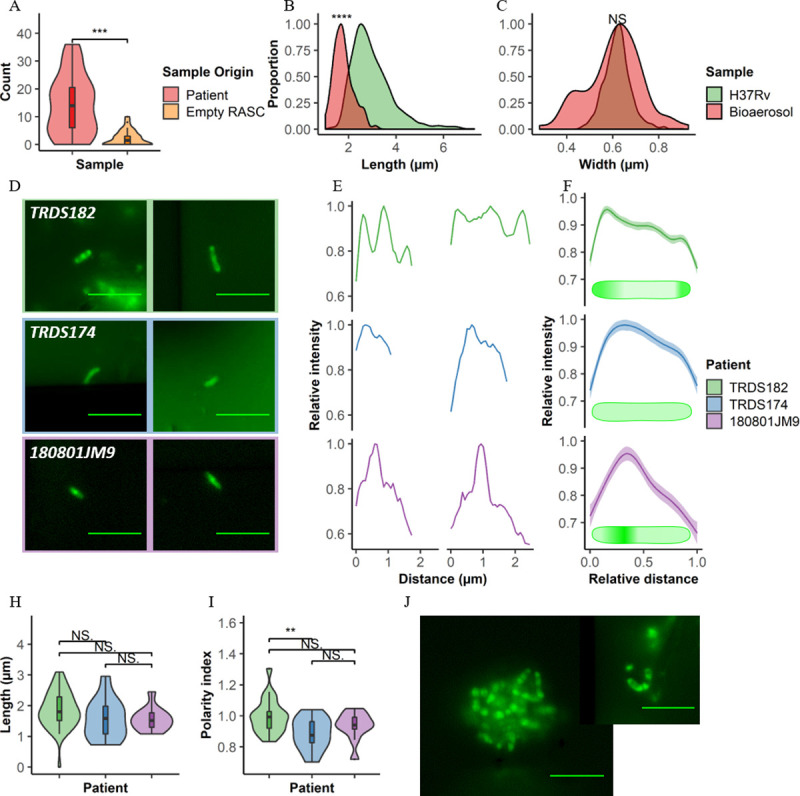
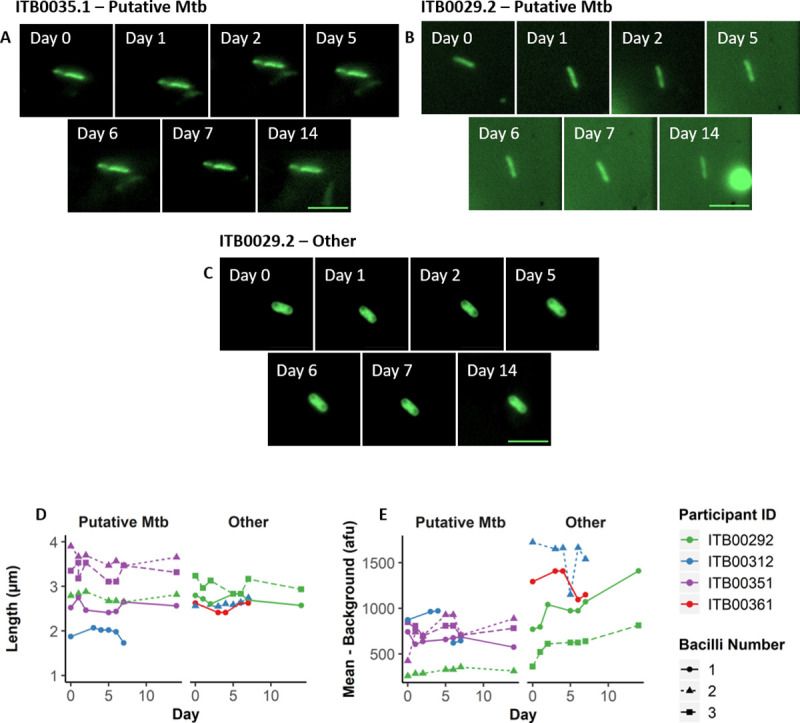
Interrupting transmission is an attractive anti-tuberculosis (TB) strategy but it remains underexplored owing to our poor understanding of the events surrounding transfer of Mycobacterium tuberculosis (Mtb) between hosts. Determining when live, infectious Mtb bacilli are released and by whom has proven especially challenging. Consequently, transmission chains are inferred only retrospectively, when new cases are diagnosed. This process, which relies on molecular analyses of Mtb isolates for epidemiological fingerprinting, is confounded by the prolonged infectious period of TB and the potential for transmission from transient exposures. We developed a Respiratory Aerosol Sampling Chamber (RASC) equipped with high-efficiency filtration and sampling technologies for liquid-capture of all particulate matter (including Mtb) released during respiration and non-induced cough. Combining the mycobacterial cell wall probe, DMN-trehalose, with fluorescence microscopy of RASC-captured bioaerosols, we detected and quantified putative live Mtb bacilli in bioaerosol samples arrayed in nanowell devices. The RASC enabled non-invasive capture and isolation of viable Mtb from bioaerosol within 24 hours of collection. A median 14 live Mtb bacilli (range 0-36) were isolated in single-cell format from 90% of confirmed TB patients following 60 minutes bioaerosol sampling. This represented a significant increase over previous estimates of transmission potential, implying that many more organisms might be released daily than commonly assumed. Moreover, variations in DMN-trehalose incorporation profiles suggested metabolic heterogeneity in aerosolized Mtb. Finally, preliminary analyses indicated the capacity for serial image capture and analysis of nanowell-arrayed bacilli for periods extending into weeks. These observations support the application of this technology to longstanding questions in TB transmission including the propensity for asymptomatic transmission, the impact of TB treatment on Mtb bioaerosol release, and the physiological state of aerosolized bacilli.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Organization. Global Tuberculosis Report. 2019.
-
- Sharma A, Hill A, Kurbatova E, van der Walt M, Kvasnovsky C, Tupasi T et al. Estimating the future burden of multidrug-resistant and extensively drug-resistant tuberculosis in India, the Philippines, Russia, and South Africa: a mathematical modelling study. Lancet Infect Dis. 2017; 17:707–715. 10.1016/S1473-3099(17)30247-5 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
