

Clinical and organizational risk factors for mortality during deterioration events among pediatric oncology patients in Latin America: A multicenter prospective cohort
- PMID: 33524166
- PMCID: PMC8248122
- DOI: 10.1002/cncr.33411
Clinical and organizational risk factors for mortality during deterioration events among pediatric oncology patients in Latin America: A multicenter prospective cohort
Abstract
Background: Hospitalized pediatric hematology-oncology (PHO) patients have frequent clinical deterioration events (CDE) requiring intensive care unit (ICU) admission, particularly in resource-limited settings. The objective of this study was to describe CDEs in hospitalized PHO patients in Latin America and to identify event-level and center-level risk factors for mortality.
Methods: In 2017, the authors implemented a prospective registry of CDEs, defined as unplanned transfers to a higher level of care, use of ICU-level interventions on the floor, or nonpalliative floor deaths, in 16 PHO centers in 10 countries. PHO hospital admissions and hospital inpatient days were also reported. This study analyzes the first year of registry data (June 2017 to May 2018).
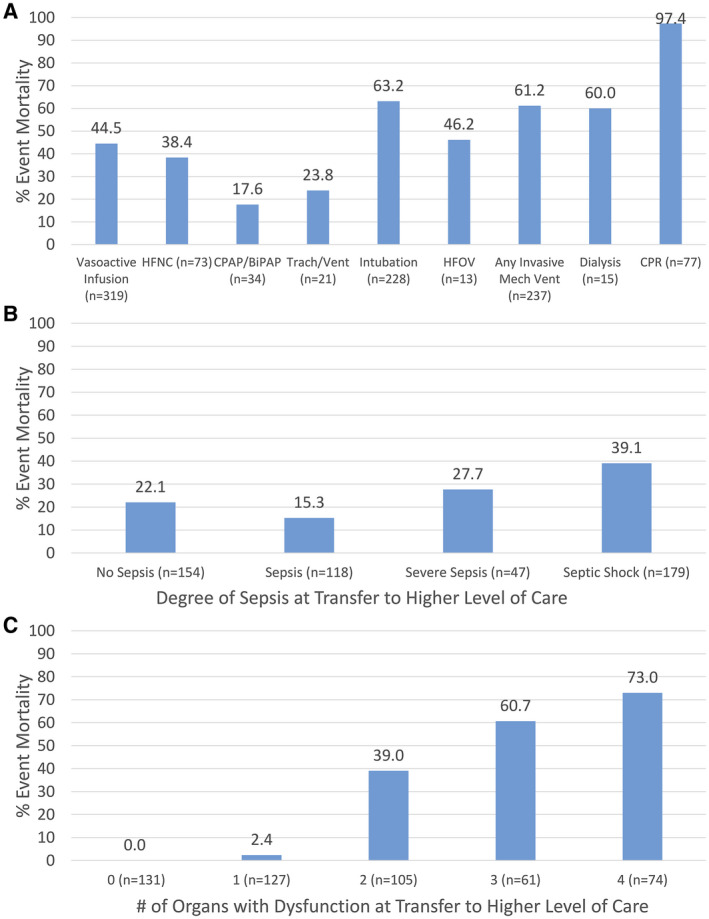
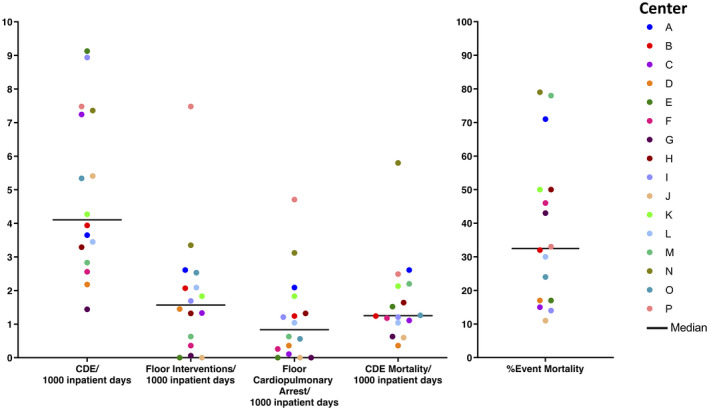
Results: Among 16 centers, 553 CDEs were reported in PHO patients during 11,536 admissions and 119,414 inpatient days (4.63 per 1000 inpatient days). Event mortality was 29% (1.33 per 1000 inpatient days) but ranged widely across centers (11%-79% or 0.36-5.80 per 1000 inpatient days). Significant risk factors for event mortality included requiring any ICU-level intervention on the floor and not being transferred to a higher level of care. Events with organ dysfunction, a higher severity of illness, and a requirement for ICU intervention had higher mortality. In center-level analysis, hospitals with a higher volume of PHO patients, less floor use of ICU intervention, lower severity of illness on transfer, and lower rates of floor cardiopulmonary arrest had lower event mortality.
Conclusions: Hospitalized PHO patients who experience CDEs in resource-limited settings frequently require floor-based ICU interventions and have high mortality. Modifiable hospital practices around the escalation of care for these high-risk patients may contribute to poor outcomes. Earlier recognition of critical illness and timely ICU transfer may improve survival in hospitalized children with cancer.
Keywords: Latin America; Pediatric Early Warning Systems (PEWS); clinical deterioration; intensive care; pediatric oncology; resource-limited settings.
© 2021 The Authors. Cancer published by Wiley Periodicals LLC on behalf of American Cancer Society.
Conflict of interest statement
The authors made no disclosures.
Figures
References
-
- Rosenman MB, Vik T, Hui SL, Breitfeld PP. Hospital resource utilization in childhood cancer. J Pediatr Hematol Oncol. 2005;27:295‐300. - PubMed
-
- Faraci M, Bagnasco F, Giardino S, et al. Intensive care unit admission in children with malignant or nonmalignant disease: incidence, outcome, and prognostic factors: a single‐center experience. J Pediatr Hematol Oncol. 2014;36:e403‐e409. - PubMed
-
- Wosten‐van Asperen RM, van Gestel JPJ, van Grotel M, et al. PICU mortality of children with cancer admitted to pediatric intensive care unit a systematic review and meta‐analysis. Crit Rev Oncol Hematol. 2019;142:153‐163. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
