

Mortality in patients admitted to intensive care with COVID-19: an updated systematic review and meta-analysis of observational studies
- PMID: 33525063
- PMCID: PMC8013495
- DOI: 10.1111/anae.15425
Mortality in patients admitted to intensive care with COVID-19: an updated systematic review and meta-analysis of observational studies
Abstract
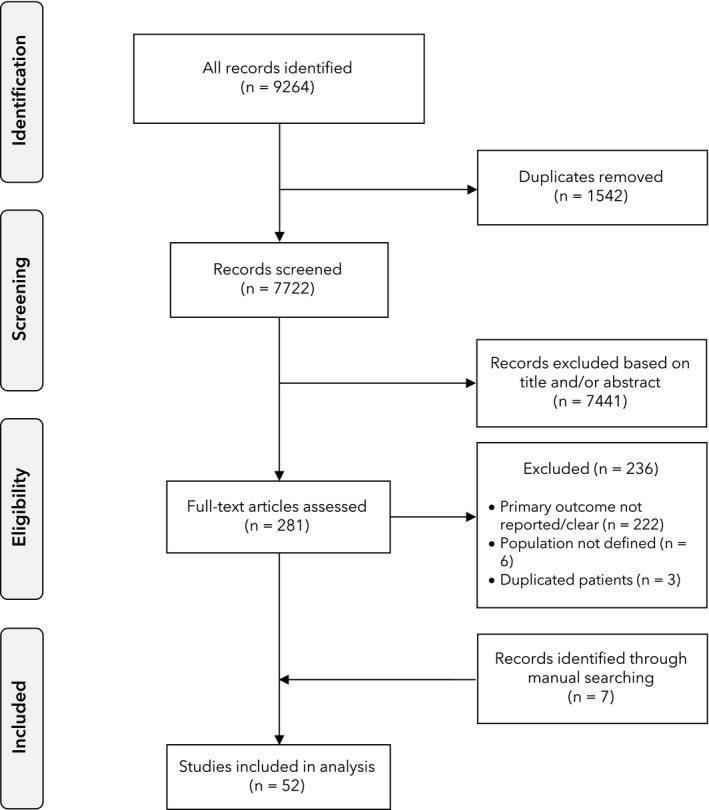
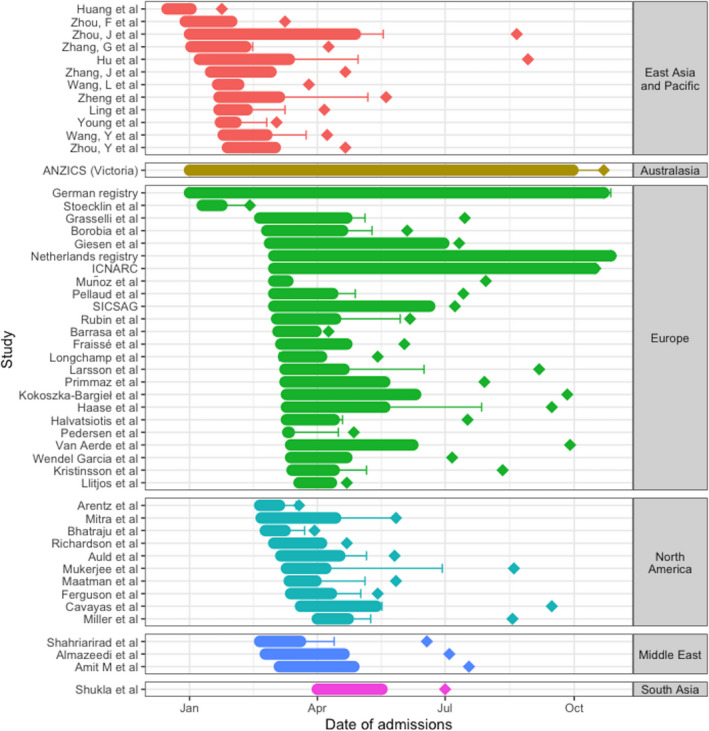
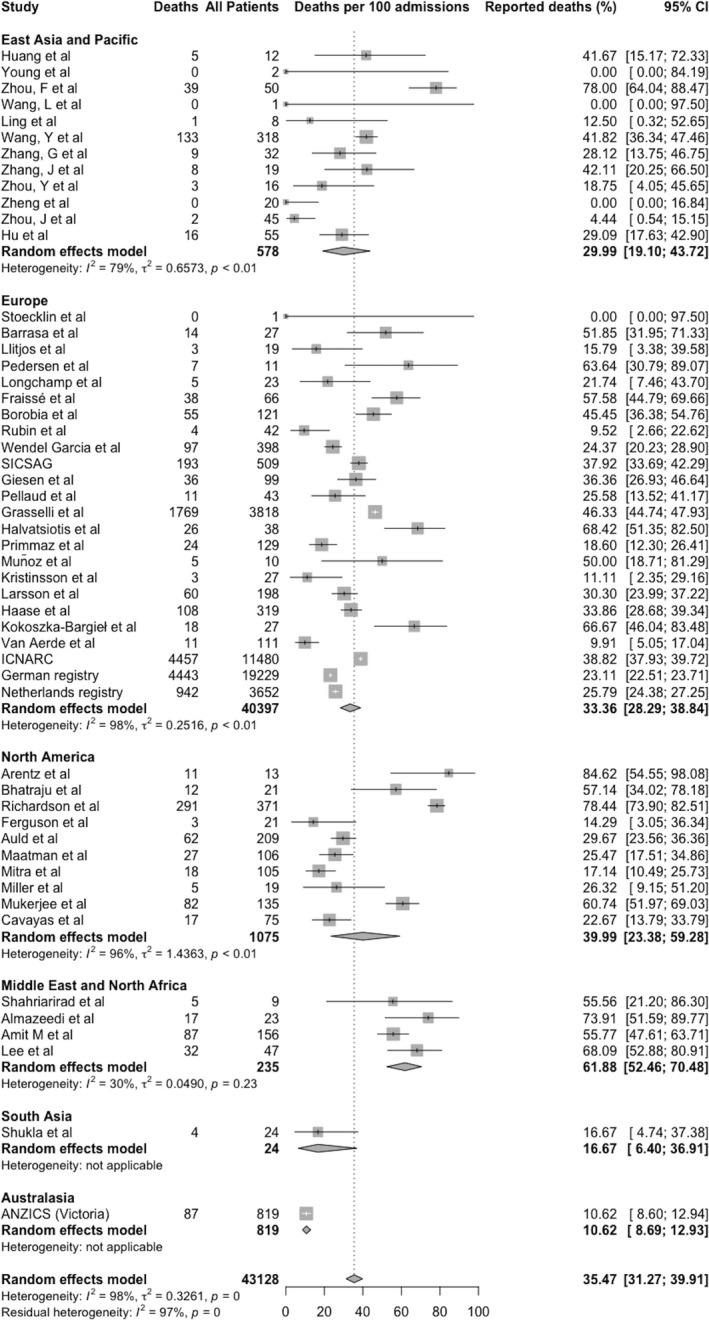
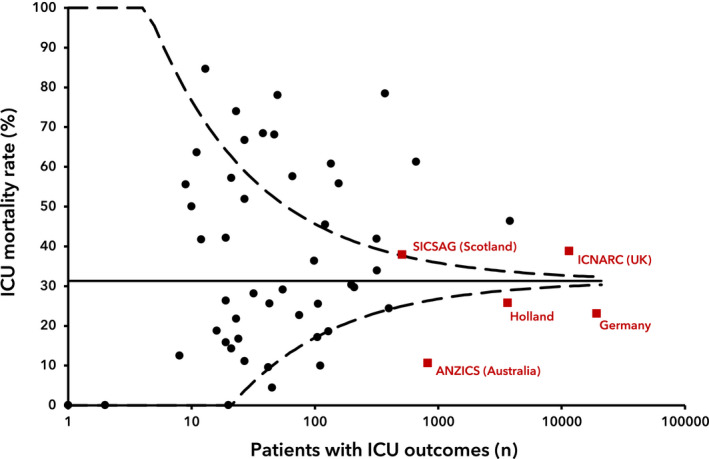
The COVID-19 pandemic continues to cause critical illness and deaths internationally. Up to 31 May 2020, mortality in patients admitted to intensive care units (ICU) with COVID-19 was 41.6%. Since then, changes in therapeutics and management may have improved outcomes. Also, data from countries affected later in the pandemic are now available. We searched MEDLINE, Embase, PubMed and Cochrane databases up to 30 September 2020 for studies reporting ICU mortality among adult patients with COVID-19 and present an updated systematic review and meta-analysis. The primary outcome measure was death in intensive care as a proportion of completed ICU admissions, either through discharge from intensive care or death. We identified 52 observational studies including 43,128 patients, and first reports from the Middle East, South Asia and Australasia, as well as four national or regional registries. Reported mortality was lower in registries compared with other reports. In two regions, mortality differed significantly from all others, being higher in the Middle East and lower in a single registry study from Australasia. Although ICU mortality (95%CI) was lower than reported in June (35.5% (31.3-39.9%) vs. 41.6% (34.0-49.7%)), the absence of patient-level data prevents a definitive evaluation. A lack of standardisation of reporting prevents comparison of cohorts in terms of underlying risk, severity of illness or outcomes. We found that the decrease in ICU mortality from COVID-19 has reduced or plateaued since May 2020 and note the possibility of some geographical variation. More standardisation in reporting would improve the ability to compare outcomes from different reports.
Keywords: COVID-19; intensive care; meta-analysis; mortality; pandemic.
© 2021 Association of Anaesthetists.
Figures
References
-
- World Health Organization . Coronavirus disease (COVID‐19) Pandemic, 2020. https://www.who.int/emergencies/diseases/novel‐coronavirus‐2019 (accessed 03/05/2020).
-
- World Health Organization . WHO Coronavirus Disease (COVID‐19) Dashboard, 2020. https://covid19.who.int/ (accessed 10/12/2020).
-
- Armstrong RA, Kane AD, Cook TM. Outcomes from intensive care in patients with COVID‐19: a systematic review and meta‐analysis of observational studies. Anaesthesia 2020; 75: 1340–9. - PubMed
-
- The RECOVERY Collaborative Group . Dexamethasone in hospitalized patients with Covid‐19 – Preliminary Report. New England Journal of Medicine 2020. Epub 17 July. 10.1056/NEJMoa2021436. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
