

Selective Surface Electrostimulation of the Denervated Zygomaticus Muscle
- PMID: 33525522
- PMCID: PMC7912406
- DOI: 10.3390/diagnostics11020188
Selective Surface Electrostimulation of the Denervated Zygomaticus Muscle
Abstract
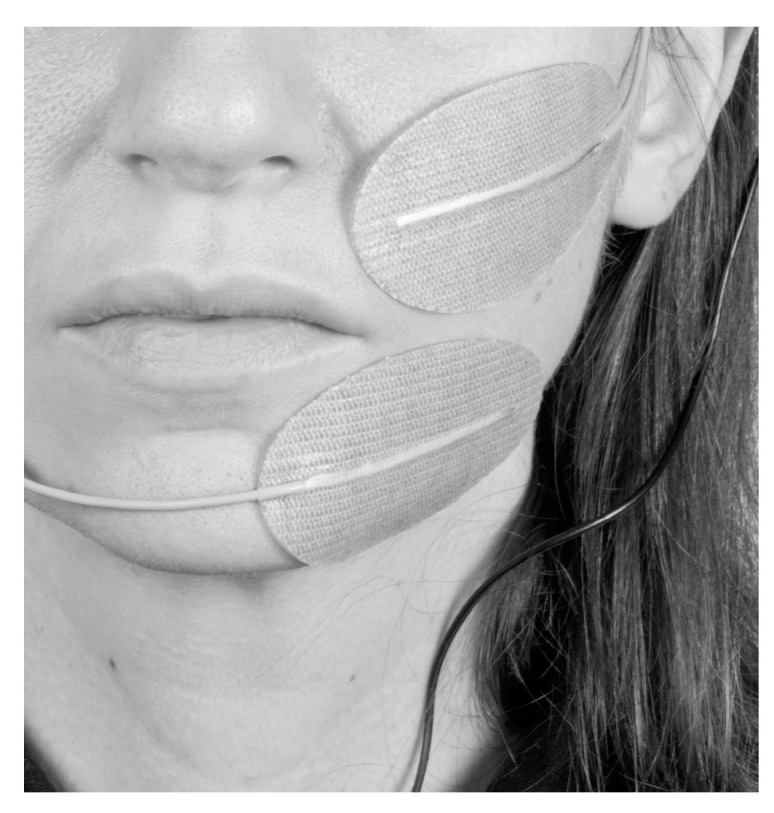
This article describes a first attempt to generate a standardized and safe selective surface electrostimulation (SES) protocol, including detailed instructions on electrode placement and stimulation parameter choice to obtain a selective stimulation of the denervated zygomaticus muscle (ZYG), without unwanted simultaneous activation of other ipsilateral or contralateral facial muscles.
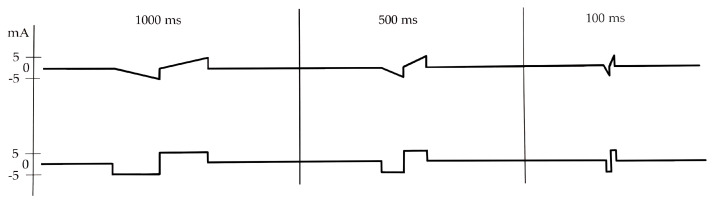
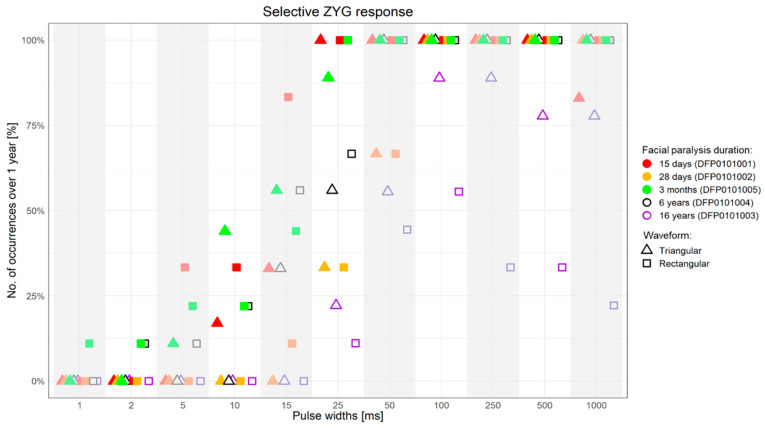
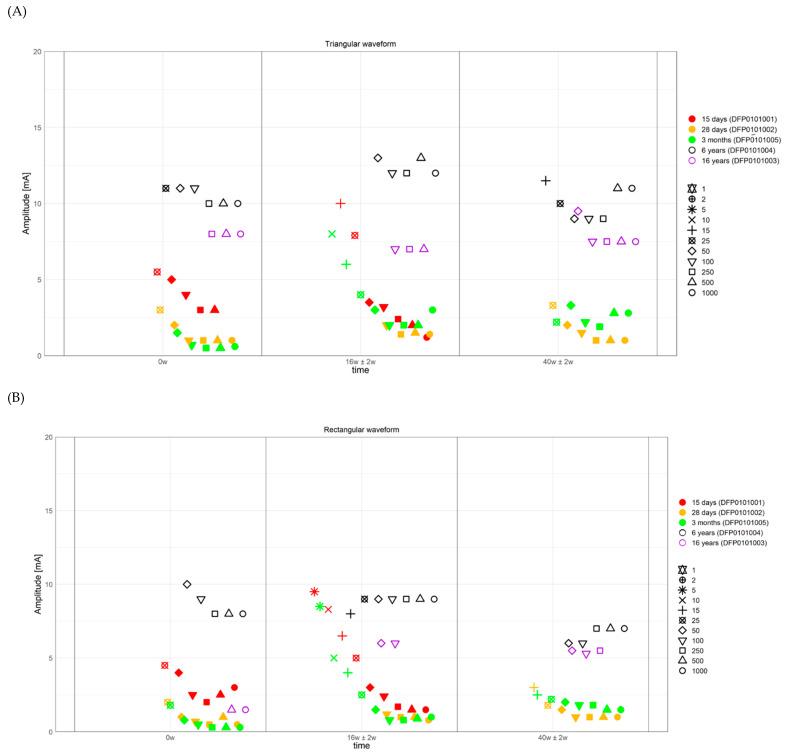
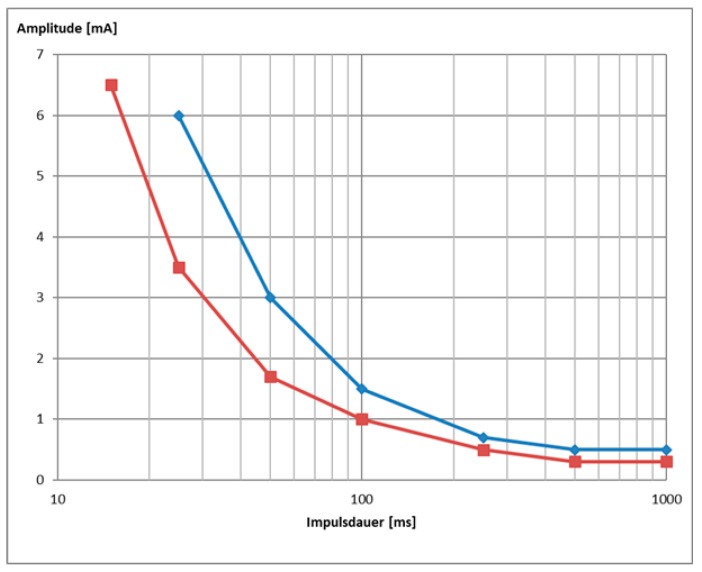
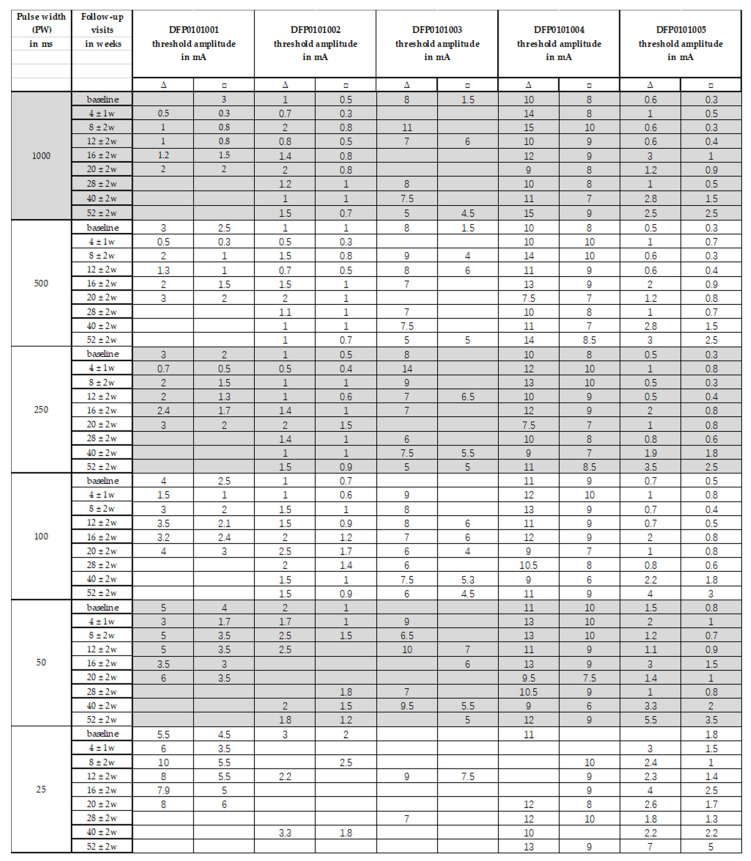
Methods: Single pulse stimulation with biphasic triangular and rectangular waveforms and pulse widths (PW) of 1000, 500, 250, 100, 50, 25, 15, 10, 5, 2, 1 ms, at increasing amplitudes between 0.1 and 20 mA was performed. Stimulations delivered in trains were assessed at a PW of 50 ms only. The stimulation was considered successful exclusively if it drew the ipsilateral corner of the mouth upwards and outwards, without the simultaneous activation of other ipsilateral or contralateral facial muscles. I/t curves, accommodation quotient, rheobase, and chronaxie were regularly assessed over 1-year follow-up.
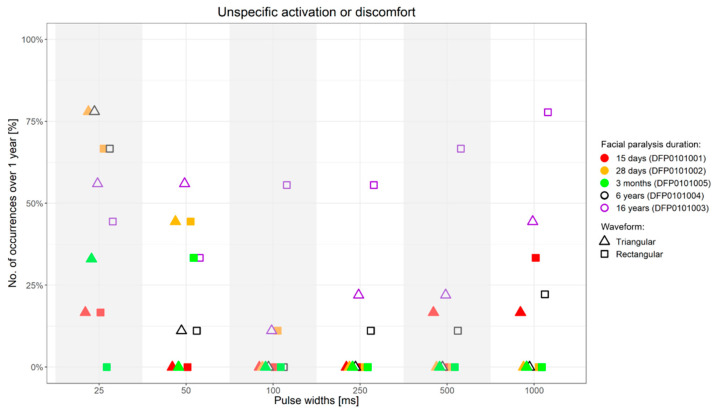
Results: 5 facial paralysis patients were assessed. Selective ZYG response in absence of discomfort and unselective contraction of other facial muscle was reproducibly obtained for all the assessed patients. The most effective results with single pulses were observed with PW ≥ 50 ms. The required amplitude was remarkably lower (≤5 mA vs. up to 15 mA) in freshly diagnosed (≤3 months) than in long-term facial paralysis patients (>5 years). Triangular was more effective than rectangular waveform, mostly because of the lower discomfort threshold of the latter. Delivery of trains of stimulation showed similar results to the single pulse setting, though lower amplitudes were necessary to achieve the selective ZYG response. Initial reinnervation signs could be detected effectively by needle-electromyography (n-EMG).
Conclusion: It is possible to define stimulation parameters able to elicit an effective selective stimulation of a specific facial muscle, in our case, of the ZYG, without causing discomfort to the patient and without causing unwanted unspecific reactions of other ipsilateral and/or contralateral facial muscles. We observed that the SES success is strongly conditioned by the correct electrode placement, which ideally should exclusively interest the area of the target muscles and its immediate proximity.
Keywords: electrostimulation; facial palsy; facial paralysis; muscle atrophy; reinnervation; surface electrodes; zygomaticus muscle.
Conflict of interest statement
The authors have no financial interest to declare in relation to the content of this article. G.F.V. and O.G.L. received research funding from MED-EL. The other authors reported no dis-closures.
Figures
Similar articles
-
Selective Electrical Surface Stimulation to Support Functional Recovery in the Early Phase After Unilateral Acute Facial Nerve or Vocal Fold Paralysis.Front Neurol. 2022 Apr 4;13:869900. doi: 10.3389/fneur.2022.869900. eCollection 2022. Front Neurol. 2022. PMID: 35444611 Free PMC article. Review.
-
Selective zygomaticus muscle activation by ball electrodes in synkinetically reinnervated patients after facial paralysis.Front Rehabil Sci. 2023 Oct 16;4:1205154. doi: 10.3389/fresc.2023.1205154. eCollection 2023. Front Rehabil Sci. 2023. PMID: 37908489 Free PMC article.
-
Tolerability of facial electrostimulation in healthy adults and patients with facial synkinesis.Eur Arch Otorhinolaryngol. 2020 Apr;277(4):1247-1253. doi: 10.1007/s00405-020-05818-x. Epub 2020 Jan 24. Eur Arch Otorhinolaryngol. 2020. PMID: 31980884 Free PMC article.
-
Altered facial muscle innervation pattern in patients with postparetic facial synkinesis.Laryngoscope. 2020 May;130(5):E320-E326. doi: 10.1002/lary.28149. Epub 2019 Jun 25. Laryngoscope. 2020. PMID: 31237361
-
Denervated muscles in humans: limitations and problems of currently used functional electrical stimulation training protocols.Artif Organs. 2002 Mar;26(3):216-8. doi: 10.1046/j.1525-1594.2002.06933.x. Artif Organs. 2002. PMID: 11940016 Review.
Cited by
-
Testosterone and long pulse width stimulation (TLPS) for denervated muscles after spinal cord injury: a study protocol of randomised clinical trial.BMJ Open. 2022 Oct 5;12(10):e064748. doi: 10.1136/bmjopen-2022-064748. BMJ Open. 2022. PMID: 36198461 Free PMC article.
-
Optimized progression of Full-Body In-Bed Gym workout: an educational case report.Eur J Transl Myol. 2023 Jun 23;33(2):11525. doi: 10.4081/ejtm.2023.11525. Eur J Transl Myol. 2023. PMID: 37358234 Free PMC article.
-
Padua Days on Muscle and Mobility Medicine, March 25-29, 2025, Hotel Petrarca, Euganean Thermae, Italy: Program and Abstracts.Eur J Transl Myol. 2025 Mar 31;35(1):13789. doi: 10.4081/ejtm.2025.13789. Epub 2025 Mar 5. Eur J Transl Myol. 2025. PMID: 40047227 Free PMC article.
-
Selective Electrical Surface Stimulation to Support Functional Recovery in the Early Phase After Unilateral Acute Facial Nerve or Vocal Fold Paralysis.Front Neurol. 2022 Apr 4;13:869900. doi: 10.3389/fneur.2022.869900. eCollection 2022. Front Neurol. 2022. PMID: 35444611 Free PMC article. Review.
-
Selective zygomaticus muscle activation by ball electrodes in synkinetically reinnervated patients after facial paralysis.Front Rehabil Sci. 2023 Oct 16;4:1205154. doi: 10.3389/fresc.2023.1205154. eCollection 2023. Front Rehabil Sci. 2023. PMID: 37908489 Free PMC article.
References
-
- Junior N., Junior J., Gignon V., Kitice A., Prado L., Santos V. Facial Nerve Palsy: Incidence of Different Ethiologies in a Tertiary Ambulatory. Int. Arch. Otorhinolaryngol. 2009;13:167–171.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
