

Clinical and endoscopic features of aorto-duodenal fistula resulting in its definitive diagnosis: an observational study
- PMID: 33526013
- PMCID: PMC7851914
- DOI: 10.1186/s12876-021-01616-9
Clinical and endoscopic features of aorto-duodenal fistula resulting in its definitive diagnosis: an observational study
Abstract
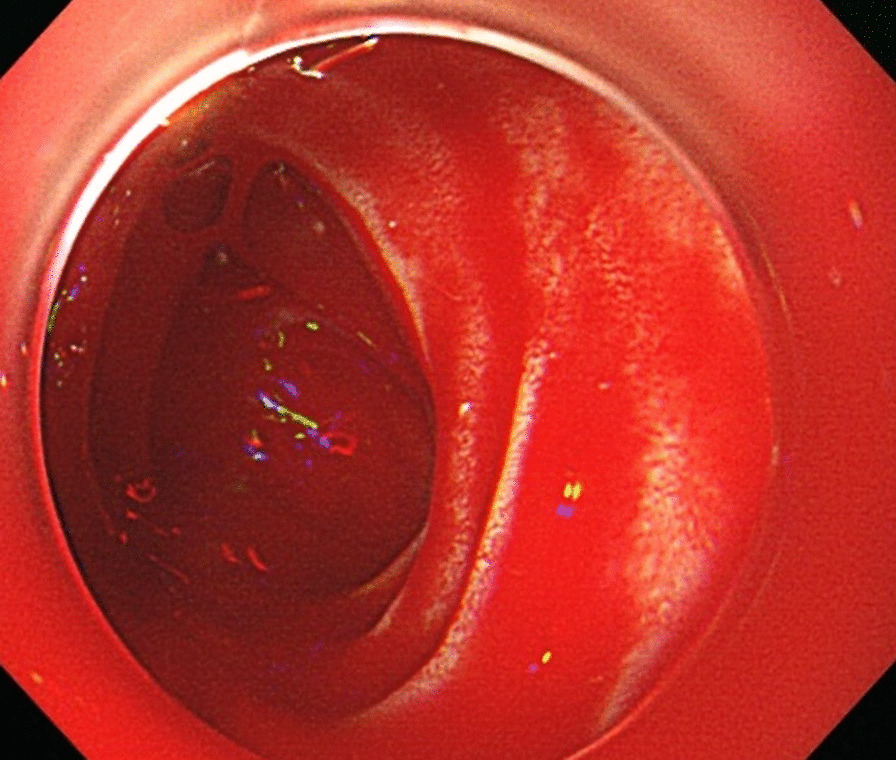
Background: Upper gastrointestinal (GI) bleeding is the most important presentation of an aorto-duodenal fistula (ADF). Early diagnosis is difficult, and the disease is associated with high mortality. The present study aimed to examine the clinical and the endoscopic characteristics of ADF in eight patients who presented to our hospital. We also sought to clarify the diagnostic approach towards the disease.
Methods: The present study examined the clinical and the endoscopic/computed tomography (CT) characteristics of ADF in eight patients who were definitively diagnosed with this condition in a 12-year period at our hospital.
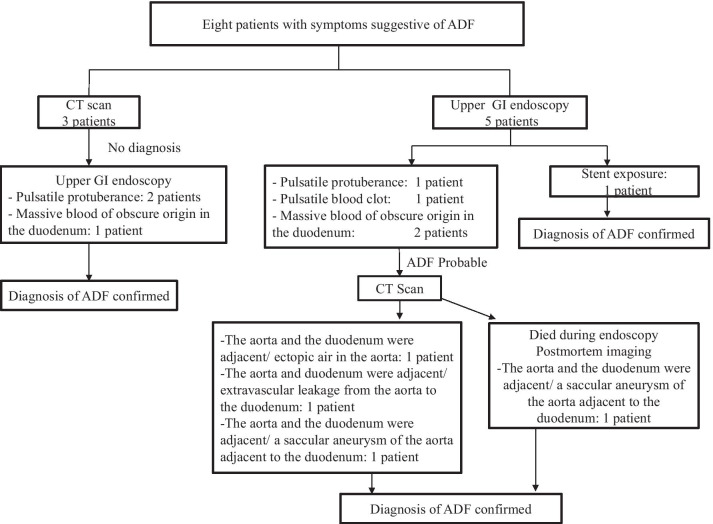
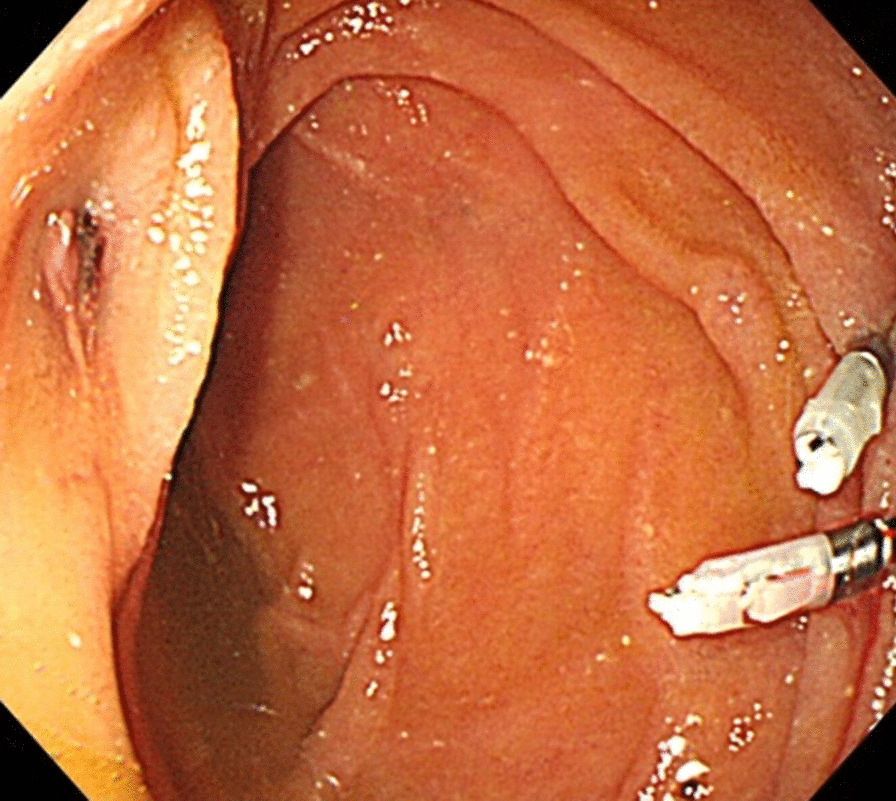
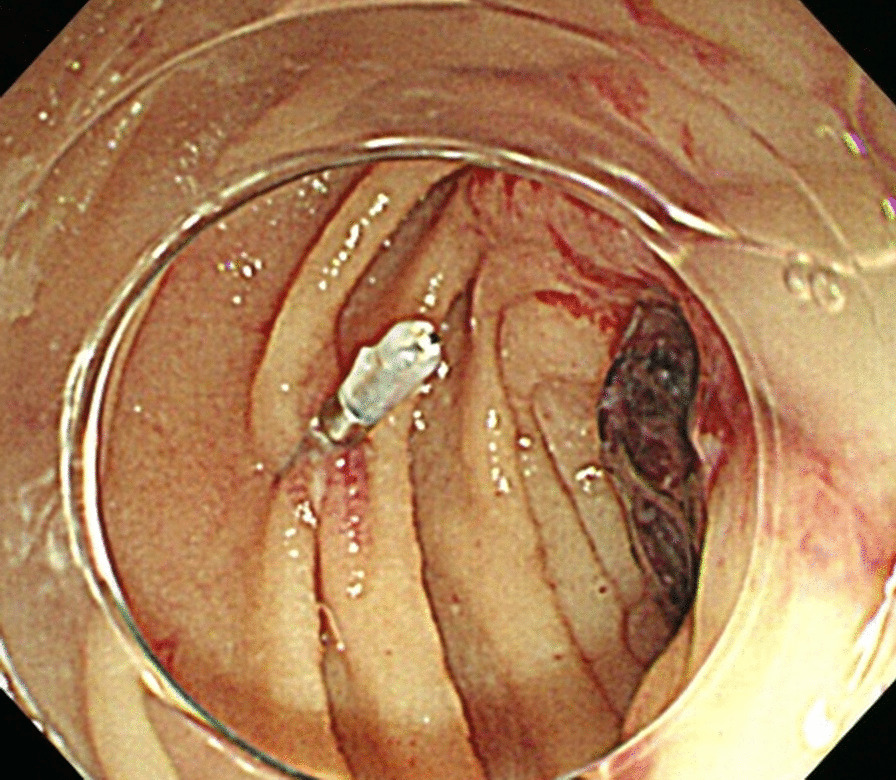
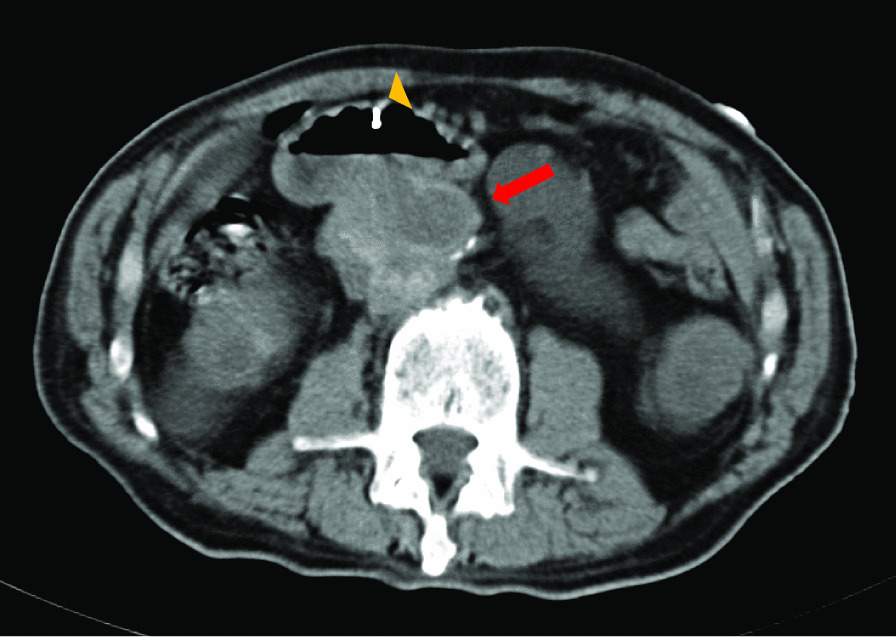
Results: The patients comprised of five men and three women, with a mean age of 69.8 years. Upper gastrointestinal bleeding was the chief complaint for all the patients. Out of these, two patients presented with shock. The patients' mean haemoglobin at presentation was 7.09 g/dL, and the mean number of blood transfusions was 7.5. All patients had undergone intervention to manage an aortic pathology in the past. As the first investigation, an upper GI endoscopy in 5 and a CT scan in 3 patients were performed. In cases where CT scan was performed first, no definitive diagnosis was obtained, and the diagnosis was confirmed by performing an upper GI endoscopy. In cases where endoscopy was performed first, definitive diagnosis was made in only one case, and the other cases were confirmed by the CT scan. In some cases, tip attachments, converting to long endoscopes, and marking clips were found useful.
Conclusions: In patients who have undergone intervention to manage an aortic pathology and have episodes of upper gastrointestinal bleeding, ADF cannot be definitively diagnosed with only one investigation. In addition, when performing upper GI endoscopy in cases where an ADF is suspected, tip attachment, converting to a long endoscope, and using marking clips can be helpful.
Keywords: Aorto-duodenal fistula; Aorto-enteric fistula; Upper gastrointestinal bleeding.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


Similar articles
-
Primary aortoduodenal fistula associated with abdominal aortic aneurysm with presentation of gastrointestinal bleeding: a case report.BMC Cardiovasc Disord. 2018 Jun 7;18(1):113. doi: 10.1186/s12872-018-0852-y. BMC Cardiovasc Disord. 2018. PMID: 29879911 Free PMC article.
-
Primary Aorto-Duodenal Fistula in Association with Chronic Ischemic Enteritis: A Case Report.Ann Vasc Surg. 2021 May;73:561-565. doi: 10.1016/j.avsg.2020.12.056. Epub 2021 Feb 5. Ann Vasc Surg. 2021. PMID: 33549790
-
Computed tomography diagnosis of primary aorto-enteric fistula.Clin Imaging. 1989 Sep;13(3):215-6. doi: 10.1016/0899-7071(89)90149-6. Clin Imaging. 1989. PMID: 2819586
-
Tuberculous aorto-duodenal fistula: a rare cause of upper gastrointestinal bleeding.Singapore Med J. 2010 May;51(5):e85-8. Singapore Med J. 2010. PMID: 20593135 Review.
-
Primary aorto-enteric fistula as a rare cause of massive gastrointestinal haemorrhage.Vasa. 2017 Oct;46(6):425-430. doi: 10.1024/0301-1526/a000646. Epub 2017 Jun 30. Vasa. 2017. PMID: 28665206 Review.
Cited by
-
Unusual cause of gastrointestinal bleeding in an 84-year-old woman: a miraculous survival from an aortoduodenal fistula repair.BMJ Case Rep. 2021 Sep 13;14(9):e244318. doi: 10.1136/bcr-2021-244318. BMJ Case Rep. 2021. PMID: 34518182 Free PMC article.
-
Secondary Aortoduodenal Fistula Diagnosed after Repeated Gastrointestinal Bleeding Episodes in a Patient With Prior Aortic Graft Surgery.DEN Open. 2025 Aug 6;6(1):e70181. doi: 10.1002/deo2.70181. eCollection 2026 Apr. DEN Open. 2025. PMID: 40777737 Free PMC article.
-
The usefulness of gel immersion endoscopy in identifying herald bleeding from an infectious aortoenteric fistula: a case report.Clin J Gastroenterol. 2024 Oct;17(5):871-875. doi: 10.1007/s12328-024-02020-y. Epub 2024 Jul 23. Clin J Gastroenterol. 2024. PMID: 39039400
-
Case report: Remedial surgical treatment of aorto-duodenal fistula with infected aneurysm after endovascular aortic repair.Front Cardiovasc Med. 2022 Oct 11;9:975871. doi: 10.3389/fcvm.2022.975871. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36304548 Free PMC article.
References
-
- Okada A, Yoshimura T, Tatsuta T, Sakuraba H, Hanabata N, Shimoyama T, et al. A case of graft-duodenal fistula 25 years after operation for aortic coarctation. J Jpn Soc Gastroenerol. 2012;109:2049–2057. - PubMed
-
- Matsuura N, Fujitani K, Nakatsuka R, Miyazaki S. Secondary aortoduodenal fistula: report of 3 cases. Jpn J Gastroenterol Surg. 2018;51:406–414. doi: 10.5833/jjgs.2017.0005. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
