

Duration of symptomatic stroke and successful reperfusion with endovascular thrombectomy for anterior circulation large vessel occlusive stroke
- PMID: 33526478
- PMCID: PMC8325713
- DOI: 10.1136/neurintsurg-2020-016961
Duration of symptomatic stroke and successful reperfusion with endovascular thrombectomy for anterior circulation large vessel occlusive stroke
Abstract
Background: It has been reported that longer time intervals from stroke onset to endovascular therapy are associated with lower rates of successful reperfusion in acute ischemic stroke patients with large vessel occlusion. However, procedural variables and potential mechanisms of this association have not been fully elucidated.
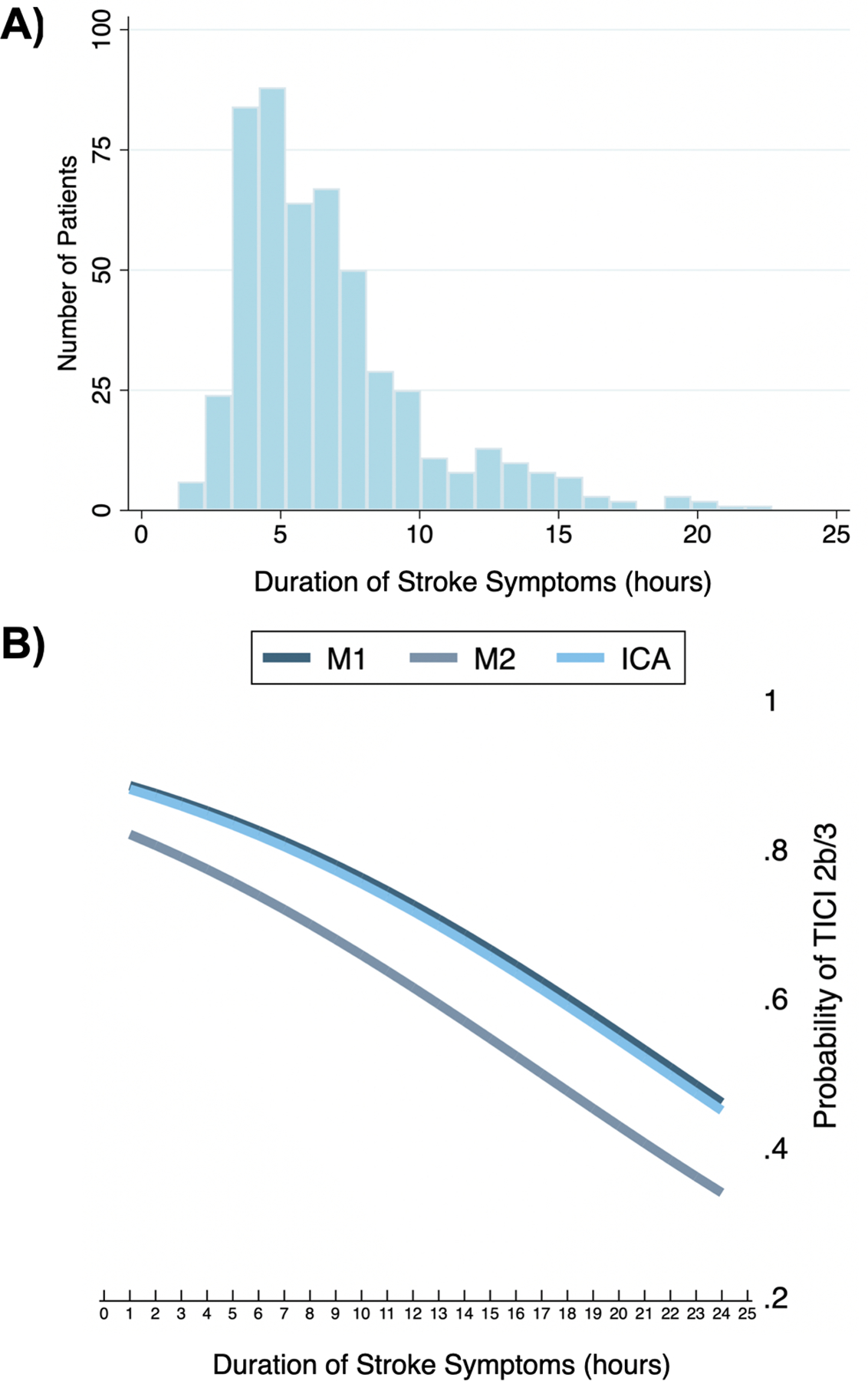
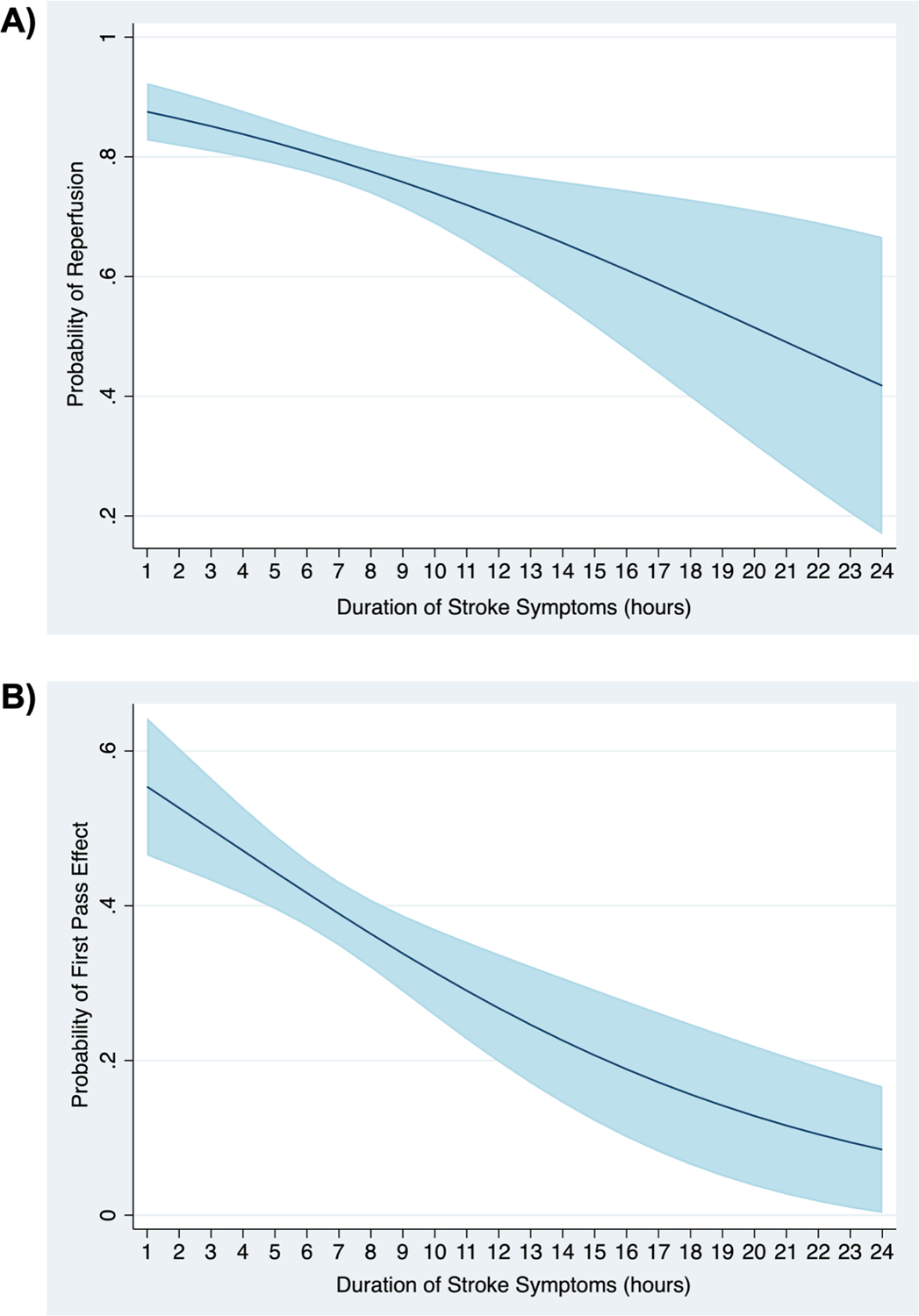
Methods: We performed a secondary analysis of individual patient data from the North American Solitaire Stent Retriever Acute Stroke (NASA) and Trevo Stent-Retriever Acute Stroke (TRACK) registries. We included patients with occlusion of the internal carotid artery or middle cerebral artery (M1 and M2 segments) who were treated by mechanical thrombectomy within 24 hours of last known normal. The primary outcome was reperfusion, defined as a Thrombolysis In Cerebral Infarction (TICI) score ≥2b. The secondary outcome was reperfusion on the first pass. The primary predictor was duration of symptomatic stroke, defined as time from last known normal to time of final pass. Adjusted logistic regression models were utilized to determine associations between variables and outcome.
Results: We included 506 patients, of which 401 (79.3%) achieved successful reperfusion (TICI 2b/3). The mean (SD) duration of symptomatic stroke was 6.8 (3.5) hours and in the adjusted logistic regression model the duration of symptomatic stroke was associated with reperfusion (OR 0.90, 95% CI 0.84 to 0.96) and reperfusion on the first pass (OR 0.89, 95% CI 0.83 to 0.95). In that model, the predicted probability of reperfusion was 88% (95% CI 0.83 to 0.92) at 1 hour, 81% (95% CI 0.78 to 0.84) at 6 hours, 70% (95% CI 0.63 to 0.77) at 12 hours, and 42% (95% CI 0.17 to 0.67) at 24 hours (ptrend=0.001). Reperfused patients were significantly younger, more likely to be male, and to have had a balloon guide catheter used during the procedure.
Conclusion: In a real-world cohort of acute ischemic stroke patients with anterior circulation occlusion treated with endovascular therapy, longer duration of symptomatic stroke is associated with lower rates of successful reperfusion and reperfusion on the first pass.
Keywords: acute ischemic stroke; endovascular thrombectomy; large vessel occlusion; neurologic outcome.
© Author(s) (or their employer(s)) 2021. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: AD reports investigator initiated funding from AMAG and Regeneron pharmaceuticals. RGN reports consulting fees for advisory roles with Anaconda, Biogen, Cerenovus, Genentech, Imperative Care, Medtronic, Phenox, Prolong Pharmaceuticals, Stryker Neurovascular and stock options for advisory roles with Astrocyte, Brainomix, Cerebrotech, Ceretrieve, Corindus Vascular Robotics, Vesalio, Viz-AI, and Perfuze. TN is Principal Investigator of the CLEAR study funded by Medtronic; serves on the Data Safety Monitoring Board for TESLA (Thrombectomy for Emergent Salvage of Large Anterior Circulation Ischemic Stroke), ENDOLOW (Endovascular Therapy for Low NIHSS Ischemic Strokes), and SELECT 2 (A Randomized Controlled Trial to Optimize Patient’s Selection for Endovascular Treatment in Acute Ischemic Stroke) trials.
Figures
References
-
- Boyle K, Joundi R, Aviv R. An historical and contemporary review of endovascular therapy for acute ischemic stroke. Neurovascular Imaging 2017;3:1–12.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical