

Breath can discriminate tuberculosis from other lower respiratory illness in children
- PMID: 33526828
- PMCID: PMC7851130
- DOI: 10.1038/s41598-021-80970-w
Breath can discriminate tuberculosis from other lower respiratory illness in children
Abstract
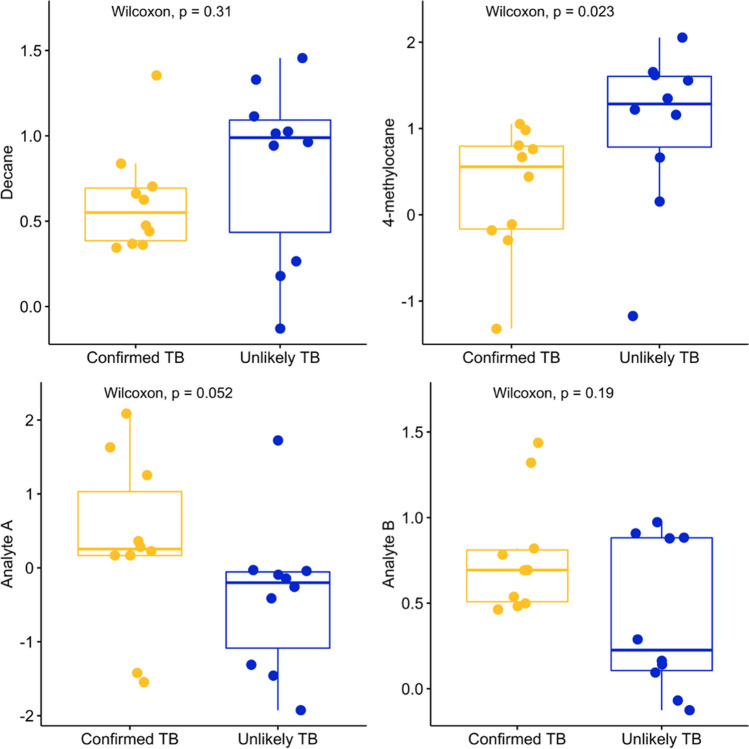
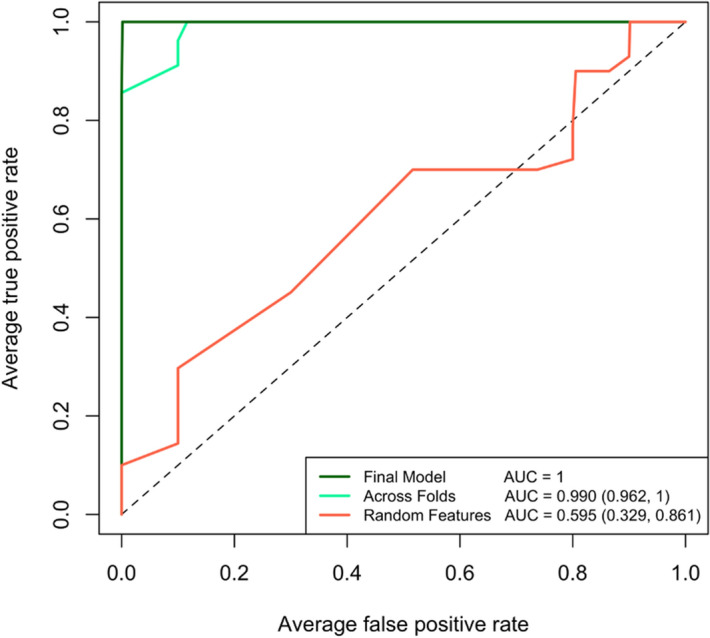
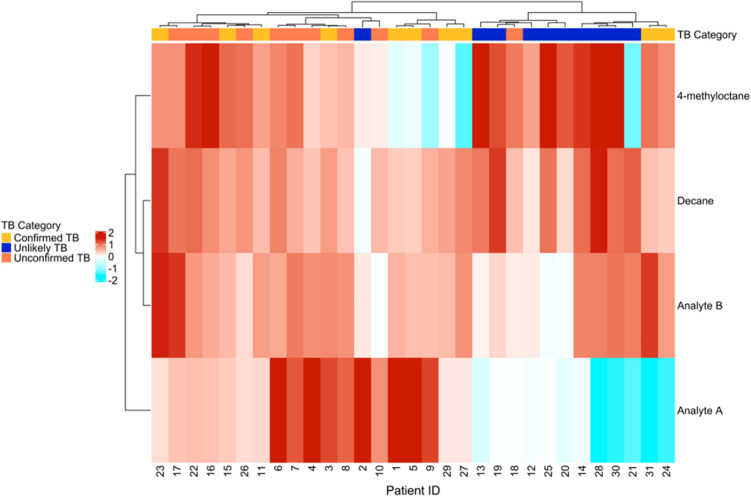
Pediatric tuberculosis (TB) remains a global health crisis. Despite progress, pediatric patients remain difficult to diagnose, with approximately half of all childhood TB patients lacking bacterial confirmation. In this pilot study (n = 31), we identify a 4-compound breathprint and subsequent machine learning model that accurately classifies children with confirmed TB (n = 10) from children with another lower respiratory tract infection (LRTI) (n = 10) with a sensitivity of 80% and specificity of 100% observed across cross validation folds. Importantly, we demonstrate that the breathprint identified an additional nine of eleven patients who had unconfirmed clinical TB and whose symptoms improved while treated for TB. While more work is necessary to validate the utility of using patient breath to diagnose pediatric TB, it shows promise as a triage instrument or paired as part of an aggregate diagnostic scheme.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- WHO Global tuberculosis report 2018. WHO (World Health Organization, Geneva, 2019).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
