

Outcomes of COVID-19 patients treated with continuous positive airway pressure outside the intensive care unit
- PMID: 33527074
- PMCID: PMC7607967
- DOI: 10.1183/23120541.00541-2020
Outcomes of COVID-19 patients treated with continuous positive airway pressure outside the intensive care unit
Abstract
Aim: We aimed to characterise a large population of coronavirus disease 2019 (COVID-19) patients with moderate-to-severe hypoxaemic acute respiratory failure (ARF) receiving continuous positive airway pressure (CPAP) outside the intensive care unit (ICU), and to ascertain whether the duration of CPAP application increased the risk of mortality for patients requiring intubation.
Methods: In this retrospective, multicentre cohort study, we included adult COVID-19 patients, treated with CPAP outside ICU for hypoxaemic ARF from 1 March to 15 April, 2020. We collected demographic and clinical data, including CPAP therapeutic goal, hospital length of stay and 60-day in-hospital mortality.
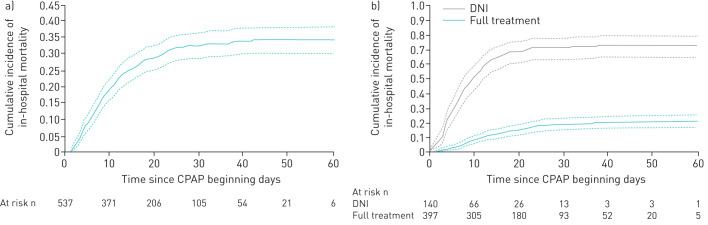
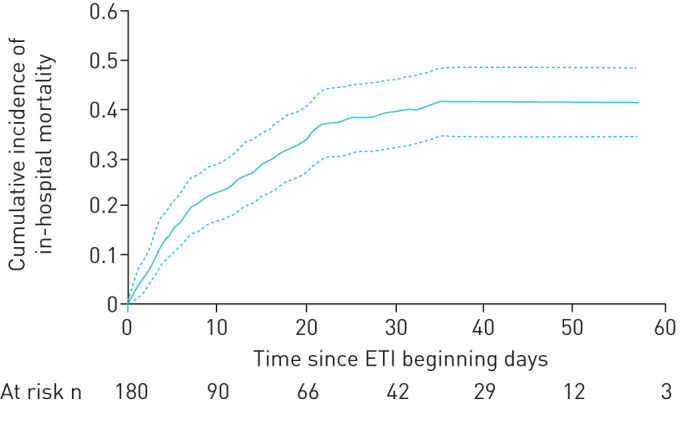
Results: The study included 537 patients with a median (interquartile range (IQR) age of 69 (60-76) years. 391 (73%) were male. According to the pre-defined CPAP therapeutic goal, 397 (74%) patients were included in the full treatment subgroup, and 140 (26%) in the do not intubate (DNI) subgroup. Median (IQR) CPAP duration was 4 (1-8) days, while hospital length of stay was 16 (9-27) days. 60-day in-hospital mortality was 34% (95% CI 0.304-0.384%) overall, and 21% (95% CI 0.169-0.249%) and 73% (95% CI 0.648-0.787%) for full treatment and DNI subgroups, respectively. In the full treatment subgroup, in-hospital mortality was 42% (95% CI 0.345-0.488%) for 180 (45%) CPAP failures requiring intubation, and 2% (95% CI 0.008-0.035%) for the remaining 217 (55%) patients who succeeded. Delaying intubation was associated with increased mortality (hazard ratio 1.093, 95% CI 1.010-1.184).
Conclusions: We described a large population of COVID-19 patients treated with CPAP outside ICU. Intubation delay represents a risk factor for mortality. Further investigation is needed for early identification of CPAP failures.
Copyright ©ERS 2021.
Conflict of interest statement
Conflict of interest: R. Vaschetto has nothing to disclose. Conflict of interest: F. Barone-Adesi has nothing to disclose. Conflict of interest: F. Racca reports personal fees from Philips Respironics outside the submitted work. Conflict of interest: C. Pissaia has nothing to disclose. Conflict of interest: C. Maestrone has nothing to disclose. Conflict of interest: D. Colombo reports personal fees for lectures from Nestlé Healthcare Nutrition outside the submitted work. Conflict of interest: C. Olivieri has a patent 102016000114357 with royalties paid to Intersurgical SpA. Conflict of interest: N. De Vita has nothing to disclose. Conflict of interest: E. Santangelo has nothing to disclose. Conflict of interest: L. Scotti has nothing to disclose. Conflict of interest: L. Castello has nothing to disclose. Conflict of interest: T. Cena has nothing to disclose. Conflict of interest: M. Taverna has nothing to disclose. Conflict of interest: L. Grillenzoni has nothing to disclose. Conflict of interest: M.A. Moschella has nothing to disclose. Conflict of interest: G. Airoldi has nothing to disclose. Conflict of interest: S. Borrè has nothing to disclose. Conflict of interest: F. Mojoli reports personal fees for lecturing from GE Healthcare, Medical and Seda Spa, outside the submitted work; and a consultancy agreement between University of Pavia and Hamilton Medical. Conflict of interest: F. Della Corte has nothing to disclose. Conflict of interest: M. Baggiani has nothing to disclose. Conflict of interest: S. Baino has nothing to disclose. Conflict of interest: P. Balbo has nothing to disclose. Conflict of interest: S. Bazzano has nothing to disclose. Conflict of interest: V. Bonato has nothing to disclose. Conflict of interest: S. Carbonati has nothing to disclose. Conflict of interest: F. Crimaldi has nothing to disclose. Conflict of interest: V. Daffara has nothing to disclose. Conflict of interest: L. De Col has nothing to disclose. Conflict of interest: M. Maestrone has nothing to disclose. Conflict of interest: M. Malerba has nothing to disclose. Conflict of interest: F. Moroni has nothing to disclose. Conflict of interest: R. Perucca has nothing to disclose. Conflict of interest: M. Pirisi has nothing to disclose. Conflict of interest: V. Rondi has nothing to disclose. Conflict of interest: D. Rosalba has nothing to disclose. Conflict of interest: L. Vanni has nothing to disclose. Conflict of interest: F. Vigone has nothing to disclose. Conflict of interest: P. Navalesi reports personal fees from Intersurgical SpA, Resmed, Philips, Novartis, MSD, Getinge and Orion Pharma, and research equipment (institutional) from Draeger, outside the submitted work; in addition, he has a patent 102020000008305 pending to Università di Padova (no profit) and a patent 102016000114357 with royalties paid to Intersurgical SpA. Conflict of interest: G. Cammarota has nothing to disclose.
Figures
References
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous