

Thermodilution-derived volumetric resting coronary blood flow measurement in humans
- PMID: 33528358
- PMCID: PMC9724906
- DOI: 10.4244/EIJ-D-20-01092
Thermodilution-derived volumetric resting coronary blood flow measurement in humans
Abstract
Background: Quantification of microvascular function requires the measurement of flow and resistance at rest and during hyperaemia. Continuous intracoronary thermodilution accurately measures coronary flow during hyperaemia.
Aims: The aim of this study was to investigate whether continuous coronary thermodilution using lower infusion rates also enables volumetric coronary blood flow measurements (in mL/min) at rest.
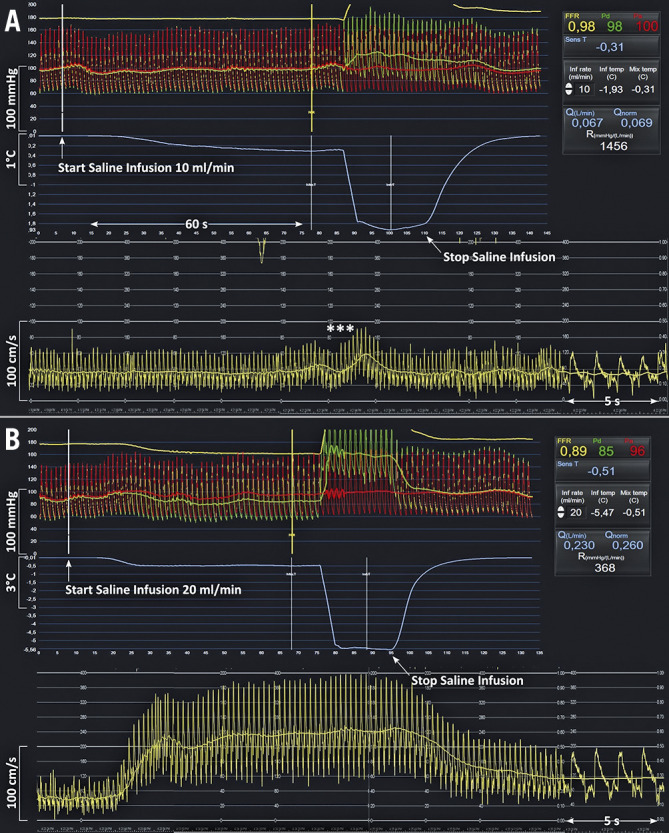
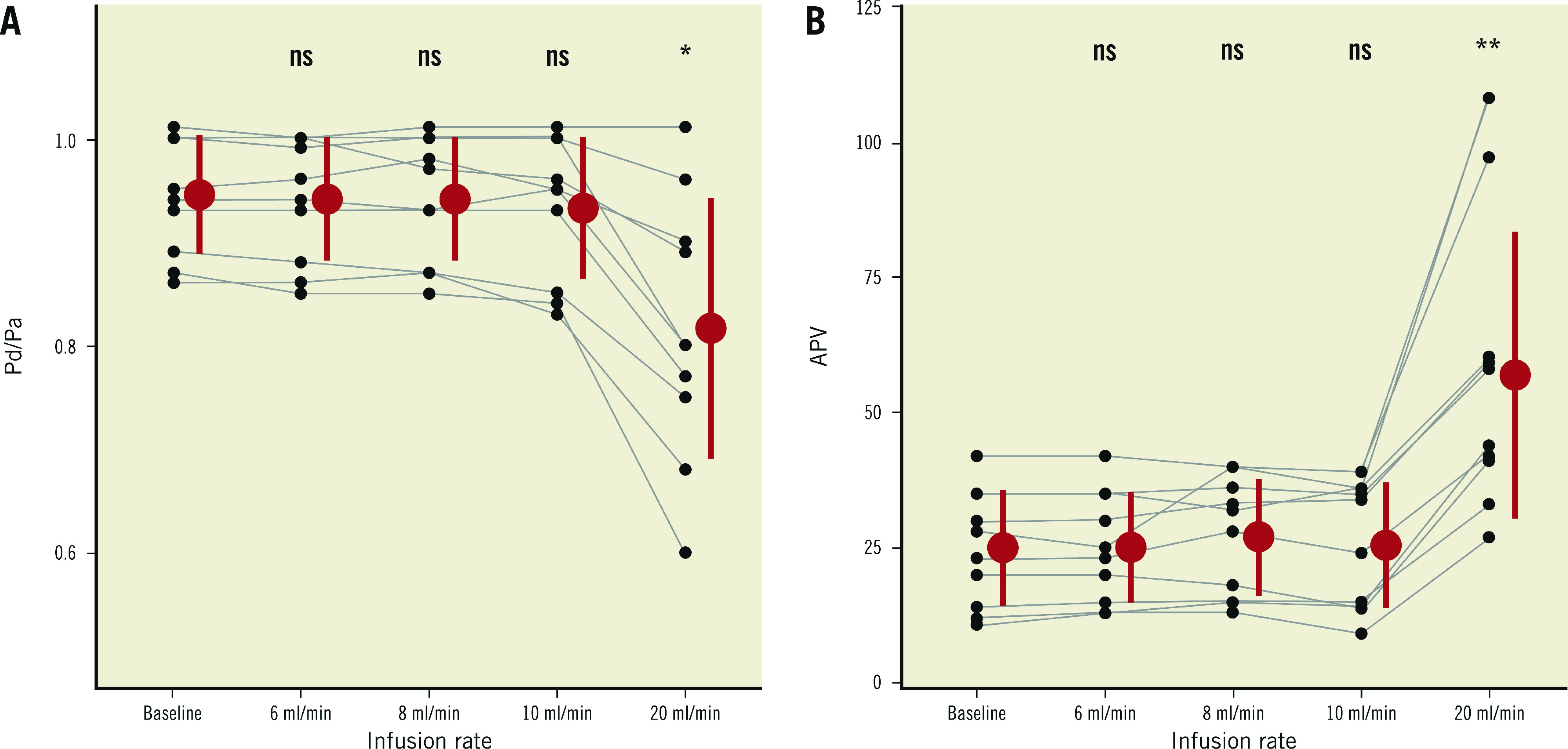
Methods: In 59 patients (88 arteries), the ratio of distal to proximal coronary pressure (Pd/Pa), as well as absolute blood flow (in mL/min) by continuous thermodilution, was recorded using a pressure/temperature guidewire. Saline was infused at rates of 10 and 20 mL/min. In 27 arteries, Doppler average peak velocity (APV) was measured simultaneously. Pd/Pa, APV, thermodilution-derived coronary flow reserve (CFRthermo) and coronary flow velocity reserve (CFVR) were assessed. In 10 arteries, simultaneous recordings were obtained at saline infusion rates of 6, 8, 10 and 20 mL/min.
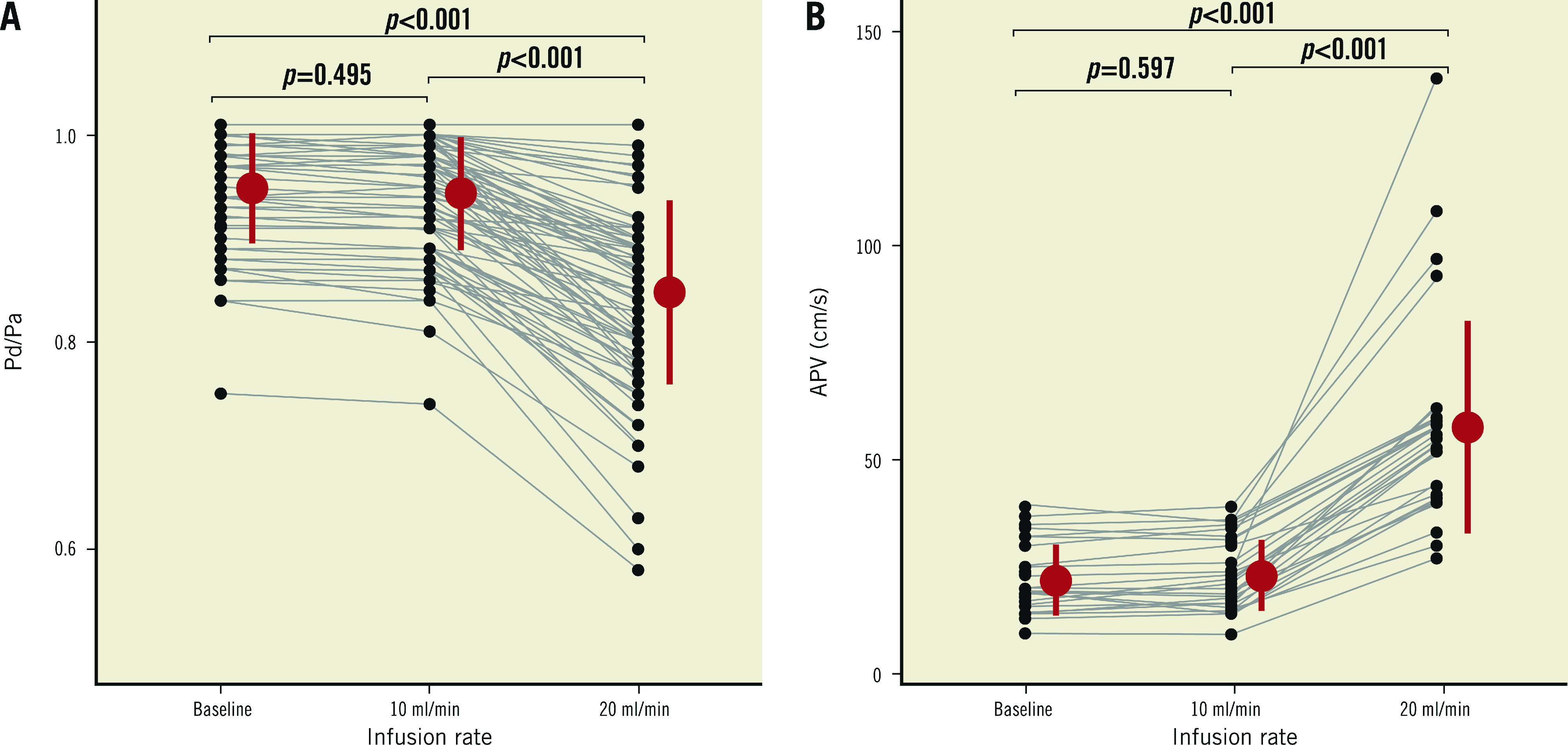
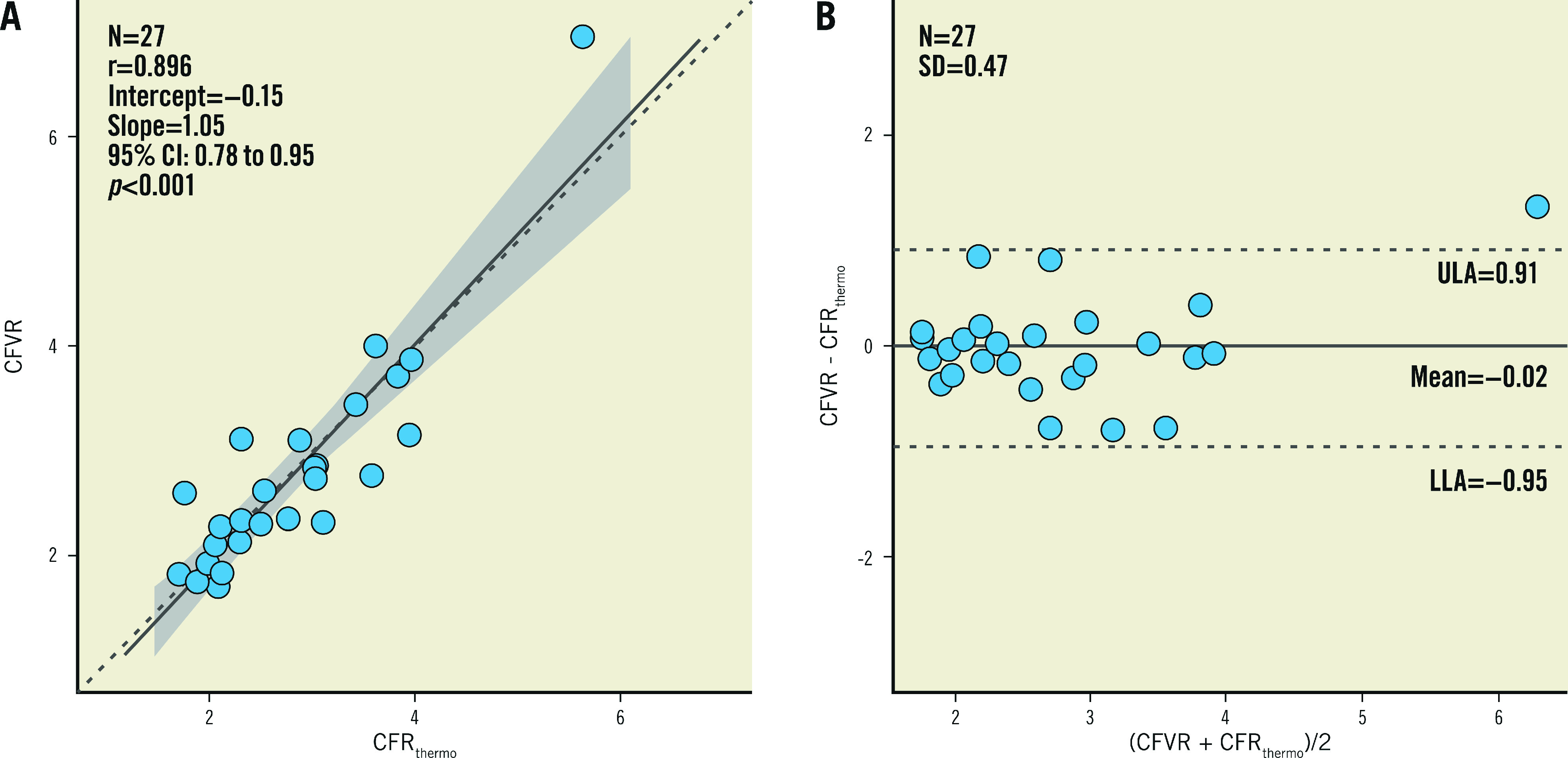
Results: Compared to baseline, saline infusion at 10 mL/min did not change Pd/Pa (0.95±0.05 versus 0.94±0.05, p=0.49) or APV (22±8 versus 23±8 cm/s, p=0.60); conversely, an infusion rate of 20 mL/min induced a decrease in Pd/Pa and an increase in APV. Stable thermodilution tracings were obtained during saline infusion at 8 and 10 mL/min, but not at 6 mL/min. Mean values of CFRthermo and CFVR were similar (2.78±0.91 versus 2.76±1.06, p=0.935) and their individual values correlated closely (r=0.89, 95% CI: 0.78-0.95, p<0.001).
Conclusions: In addition to hyperaemic flow, continuous thermodilution can quantify absolute resting coronary blood flow; therefore, it can be used to calculate coronary flow reserve and microvascular resistance reserve.
Conflict of interest statement
C. Collet reports receiving research grants from Biosensors, HeartFlow Inc., Shockwave Medical, Pie Medical, Siemens, Medis Medical Imaging and Abbott Vascular, and consultancy fees from Opsens, Boston Scientific, Medyria, HeartFlow Inc., and Philips/Volcano. B. De Bruyne has received grants from Abbott Vascular, Boston Scientific and Biotronik, institutional consulting fees from Abbott and Boston Scientific, and is a shareholder in Philips, Siemens, GE, Bayer, HeartFlow, Edwards Lifesciences, and Ceyliad. S. Fournier declares speaker fees from Bayer, Amgen, and Biotronik, and consulting fees (advisory boards) from Bayer, and CathWorks. M. van ’t Veer declares speaker fees from Abbott. N. Pijls declares institutional research grants from Abbott and Hexacath, consultancy for Abbott, Opsens and General Electric, and minor equity in Philips, ASML, HeartFlow and GE. The other authors have no conflicts of interest to declare.
Figures
References
-
- Aarnoudse W, Van’t Veer M, Pijls NH, Ter Woorst J, Vercauteren S, Tonino P, Geven M, Rutten M, van Hagen E, De Bruyne B, Van De Vosse F. Direct volumetric blood flow measurement in coronary arteries by thermodilution. J Am Coll Cardiol. 2007;50:2294–304. doi: 10.1016/j.jacc.2007.08.047. - DOI - PubMed
-
- Xaplanteris P, Fournier S, Keulards DCJ, Adjedj J, Ciccarelli G, Milkas A, Pellicano M, Veer M, Barbato E, Pijls NHJ, Bruyne BD. Catheter-based measurements of absolute coronary blood flow and microvascular resistance. Circ Cardiovasc Interv. 2018;11:e006194. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical