

Extracorporeal membrane oxygenation in patients with severe respiratory failure from COVID-19
- PMID: 33528595
- PMCID: PMC7851810
- DOI: 10.1007/s00134-020-06331-9
Extracorporeal membrane oxygenation in patients with severe respiratory failure from COVID-19
Abstract
Purpose: Limited data are available on venovenous extracorporeal membrane oxygenation (ECMO) in patients with severe hypoxemic respiratory failure from coronavirus disease 2019 (COVID-19).
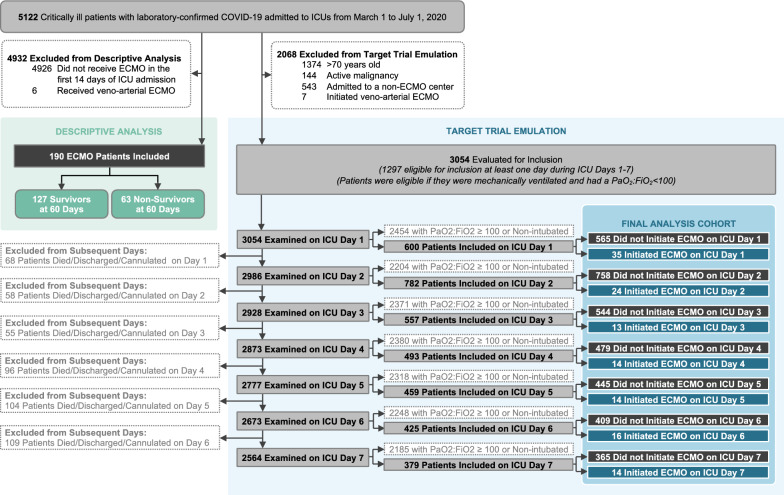
Methods: We examined the clinical features and outcomes of 190 patients treated with ECMO within 14 days of ICU admission, using data from a multicenter cohort study of 5122 critically ill adults with COVID-19 admitted to 68 hospitals across the United States. To estimate the effect of ECMO on mortality, we emulated a target trial of ECMO receipt versus no ECMO receipt within 7 days of ICU admission among mechanically ventilated patients with severe hypoxemia (PaO2/FiO2 < 100). Patients were followed until hospital discharge, death, or a minimum of 60 days. We adjusted for confounding using a multivariable Cox model.
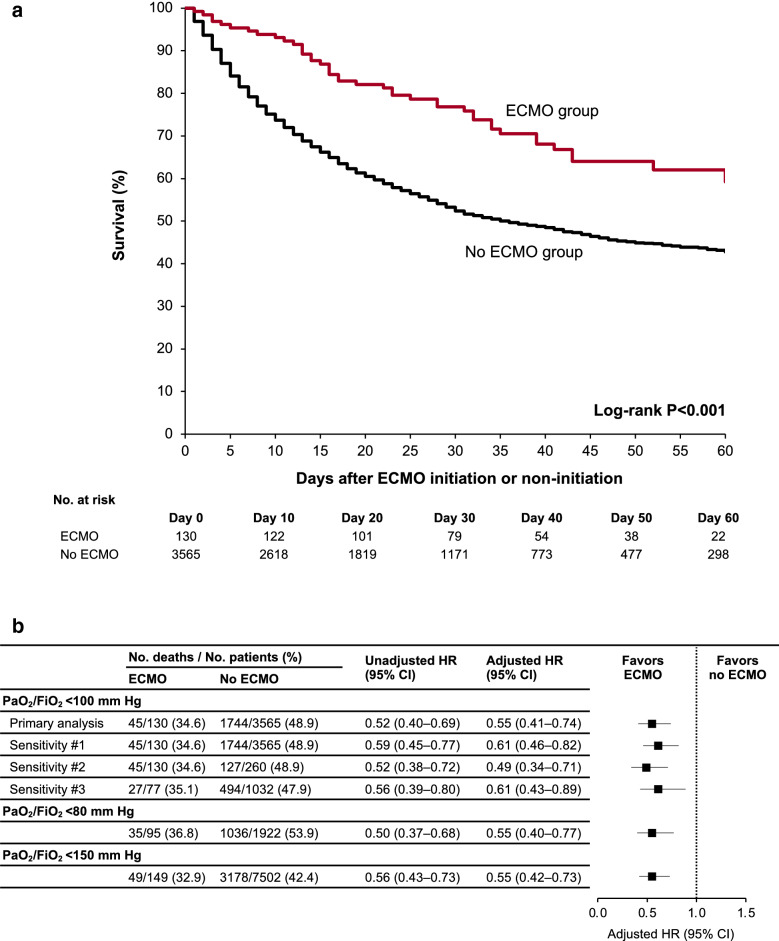
Results: Among the 190 patients treated with ECMO, the median age was 49 years (IQR 41-58), 137 (72.1%) were men, and the median PaO2/FiO2 prior to ECMO initiation was 72 (IQR 61-90). At 60 days, 63 patients (33.2%) had died, 94 (49.5%) were discharged, and 33 (17.4%) remained hospitalized. Among the 1297 patients eligible for the target trial emulation, 45 of the 130 (34.6%) who received ECMO died, and 553 of the 1167 (47.4%) who did not receive ECMO died. In the primary analysis, patients who received ECMO had lower mortality than those who did not (HR 0.55; 95% CI 0.41-0.74). Results were similar in a secondary analysis limited to patients with PaO2/FiO2 < 80 (HR 0.55; 95% CI 0.40-0.77).
Conclusion: In select patients with severe respiratory failure from COVID-19, ECMO may reduce mortality.
Keywords: ARDS; COVID-19; Extracorporeal membrane oxygenation; Mortality; Severe respiratory failure; VV-ECMO.
Conflict of interest statement
DEL received research support from BioPorto outside the submitted work. DMC reports grants and personal fees from NovoNordisk, personal fees from PLC medical, grants from Bioporto, personal fees from Fresenius, personal fees from AstraZeneca, grants and personal fees from Jannssen, grants and personal fees from Gilead, and personal fees from Merck, all outside the submitted work. AS reports personal fees from Horizon Therapeutics PLC, AstraZeneca, and CVS Caremark. SG is a scientific coordinator for the ASCEND trial (GlaskoSmithKline), outside the submitted work. KSM reports serving on the BREATHE Trial Steering Committee, funded by Roivant/Kinevant Sciences, outside the submitted work. BOG receives consulting fees from Sedana Medical outside the submitted work. The authors of the writing committee are supported by the following grants from the National Institutes of Health: K08GM134220 and R03AG060179 (SS); R01HL144566 and R01DK125786 (DEL); K23HL130648 (KSM); R37 AI102634 (MAH); F32DC017342 (SG); K23DK120811 (AS); K23HL143053 (MWS).
Figures
References
-
- Johns Hopkins University & Medicine-Coronavirus Resource Center. https://coronavirus.jhu.edu/map.html. Accessed 29 Nov 2020
-
- Bartlett RH, Ogino MT, Brodie D, McMullan DM, Lorusso R, MacLaren G, Stead CM, Rycus P, Fraser JF, Belohlavek J, Salazar L, Mehta Y, Raman L, Paden ML. Initial ELSO guidance document: ECMO for COVID-19 patients with severe cardiopulmonary failure. ASAIO J. 2020;66(5):472–474. doi: 10.1097/MAT.0000000000001173. - DOI - PMC - PubMed
-
- Abrams D, Schmidt M, Pham T, Beitler JR, Fan E, Goligher EC, McNamee JJ, Patroniti N, Wilcox ME, Combes A, Ferguson ND, McAuley DF, Pesenti A, Quintel M, Fraser J, Hodgson CL, Hough CL, Mercat A, Mueller T, Pellegrino V, Ranieri VM, Rowan K, Shekar K, Brochard L, Brodie D. Mechanical ventilation for acute respiratory distress syndrome during extracorporeal life support. Research and practice. Am J Respir Crit Care Med. 2020;201(5):514–525. doi: 10.1164/rccm.201907-1283CI. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
- K23 HL143053/HL/NHLBI NIH HHS/United States
- K23 DK116967/DK/NIDDK NIH HHS/United States
- R01 HL144566/HL/NHLBI NIH HHS/United States
- R01 DK125786/DK/NIDDK NIH HHS/United States
- R03 AG060179/AG/NIA NIH HHS/United States
- L60 DK126281/DK/NIDDK NIH HHS/United States
- K23 DK124644/DK/NIDDK NIH HHS/United States
- R01 DK128012/DK/NIDDK NIH HHS/United States
- K08 GM134220/GM/NIGMS NIH HHS/United States
- F32 DC017342/DC/NIDCD NIH HHS/United States
- R01 HL153384/HL/NHLBI NIH HHS/United States
- R37 AI102634/AI/NIAID NIH HHS/United States
- K23 HL130648/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
