

Fibrosis Regression After Eradication of Hepatitis C Virus: From Bench to Bedside
- PMID: 33529675
- PMCID: PMC8601597
- DOI: 10.1053/j.gastro.2020.09.065
Fibrosis Regression After Eradication of Hepatitis C Virus: From Bench to Bedside
Abstract
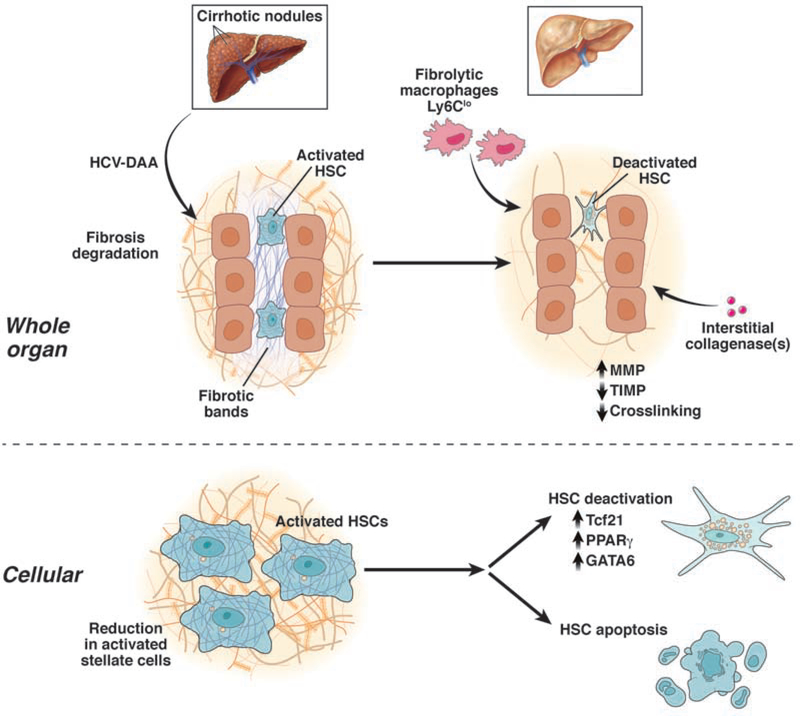
Hepatitis C virus (HCV) infection and its complications have been the major cause of cirrhosis and its complications for several decades in the Western world. Until recently, treatment for HCV with interferon-based regimens was associated with moderate success but was difficult to tolerate. More recently, however, an arsenal of novel and highly effective direct-acting antiviral (DAA) drugs has transformed the landscape by curing HCV in a broad range of patients, including those with established advanced fibrosis, cirrhosis, comorbidities, and even those with complications of cirrhosis. Fibrosis is a dynamic process comprising both extracellular matrix deposition, as well as its degradation. With almost universal sustained virologic response (SVR) (ie, elimination of HCV), it is timely to explore whether HCV eradication can reverse fibrosis and cirrhosis. Indeed, fibrosis in several types of liver disease is reversible, including HCV. However, we do not know with certainty in whom fibrosis regression can be expected after HCV elimination, how quickly it occurs, and whether antifibrotic therapies will be indicated in those with persistent cirrhosis. This review summarizes the evidence for reversibility of fibrosis and cirrhosis after HCV eradication, its impact on clinical outcomes, and therapeutic prospects for directly promoting fibrosis regression in patients whose fibrosis persists after SVR.
Keywords: Direct-Acting Antiviral; Fibrosis Regression; Hepatitis C Virus; Sustained Virologic Response.
Copyright © 2021 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures


References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
