

Effect of myocardial dysfunction in cardiac morbidity and all cause mortality in childhood cancer subjects treated with anthracycline therapy
- PMID: 33530141
- PMCID: PMC7837140
- DOI: 10.1186/s40959-015-0005-8
Effect of myocardial dysfunction in cardiac morbidity and all cause mortality in childhood cancer subjects treated with anthracycline therapy
Abstract
Background: Subacute cardiotoxicity, consisting of acute myocyte damage and associated left ventricular dysfunction, occurs early during anthracycline therapy. We investigated the impact of myocardial dysfunction, defined herein by a shortening fraction (SF) < 29 % at any time during or after anthracycline therapy, on late onset cardiomyopathy and all-cause mortality, among childhood cancer survivors exposed to anthracyclines. In addition, we sought to identify subpopulations of subjects at highest risk for cardiomyopathy and death from all causes.
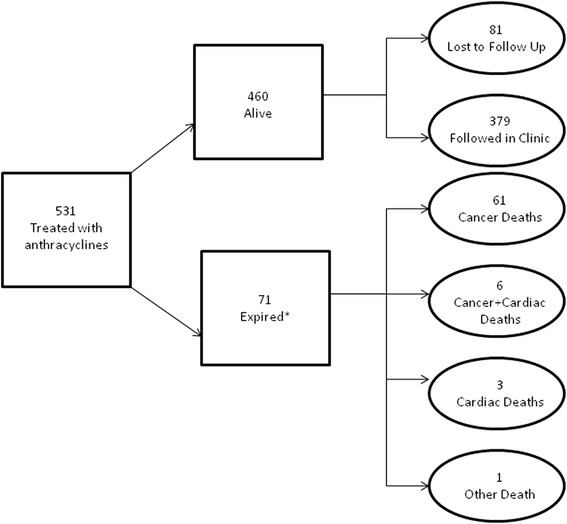
Methods: Five hundred thirty-one childhood cancer survivors exposed to anthracyclines were enrolled and studied on average 10 (1.4-27.3) years following their initial exposure. The medical records were reviewed to identify known risk factors associated with cardiotoxicity, including cumulative anthracycline dose, length of post-therapy interval, administration of other cardiotoxic medications (vinca alkaloids), previous heart disease, radiation dose to the heart, history of bone marrow transplantation, age at treatment, gender, systolic dysfunction, and history of congestive heart failure during anthracycline therapy.
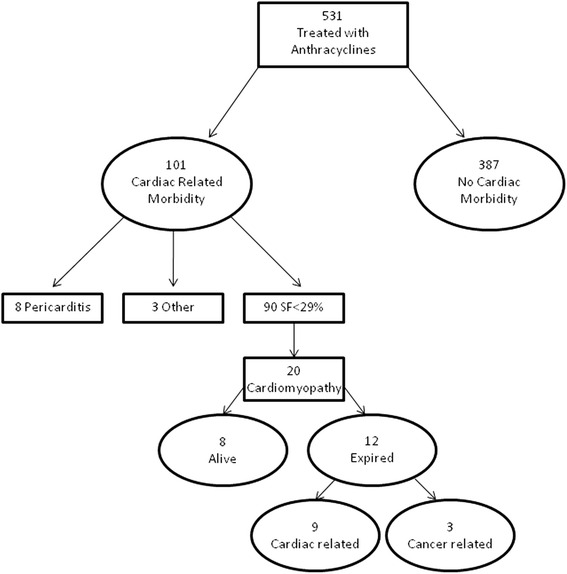
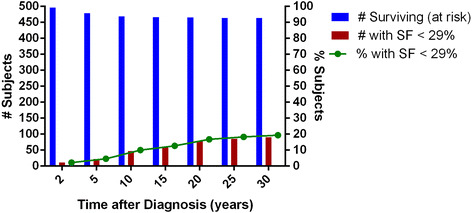
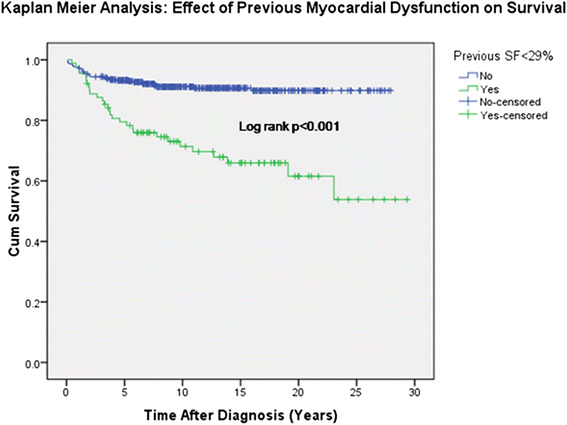
Results: Ninety subjects (16.9 %) developed SF < 29 % and 71 patients (13.4 %) died on average 10 years after initial exposure (range 1.4-27.3 years). Total cumulative dose (OR 3.27, 95 % CI 1.94, 5.49, p < 0.001) and bone marrow transplantation (OR 2.57, 95 % CI 1.24, 5.30, p = 0.01) were found to be statistically significant risk factors for development of myocardial dysfunction. There was a 3-fold increase in the odds of having a SF < 29 % at any point during or following cancer therapy if a subject underwent bone marrow transplantation or had a total cumulative dose anthracycline therapy ≥ 240 mg/m2. The all-cause mortality ratio was almost seven-fold higher (95 % CI, 2.40-fold to 17.81-fold higher) if a subject developed systolic dysfunction, defined by a previous SF < 29 % anytime during or after anthracycline therapy. Nine deaths (12.7 %) were attributed to cardiovascular disease. The risk of dying as a result of cardiac disease also was significantly higher in individuals who had a SF < 29 % at any time during or after therapy.
Conclusions: This study demonstrates an almost seven-fold increase in all cause mortality in pediatric cancer survivors with a history of anthracycline induced myocardial dysfunction defined as SF < 29 %.
Keywords: Anthracyclines; Cardiomyopathy; Cardiotoxicity.
Figures
References
-
- Billingham ME, Mason JW, Bristow MR, Daniels JR. Anthracycline cardiomyopathy monitored by morphologic changes. Cancer Treat Rep. 1978;62:865–72. - PubMed
LinkOut - more resources
Full Text Sources