

Rationale for setting up a cardio-oncology unit: our experience at Mayo Clinic
- PMID: 33530144
- PMCID: PMC7837147
- DOI: 10.1186/s40959-016-0014-2
Rationale for setting up a cardio-oncology unit: our experience at Mayo Clinic
Abstract
Background: The diagnosis and management of cardiovascular complications have become a clinical concern for oncologists, cardiologists, surgeons, interventional radiologists, radiation therapy physicians, internists, nurses, pharmacists, administrators, and all the stakeholders involved in the care of cancer patients. Anticancer therapies have extended the lives of patients with cancer, but for some this benefit is attenuated by adverse cardiovascular effects.
Methods: This review article aims to provide an overview of the rationale of setting up a cardio-oncology unit and reflect on our own experience establishing this service, and conclude with some fundamental aspects of consideration for evaluation and management of patients with cancer and cardiovascular diseases.
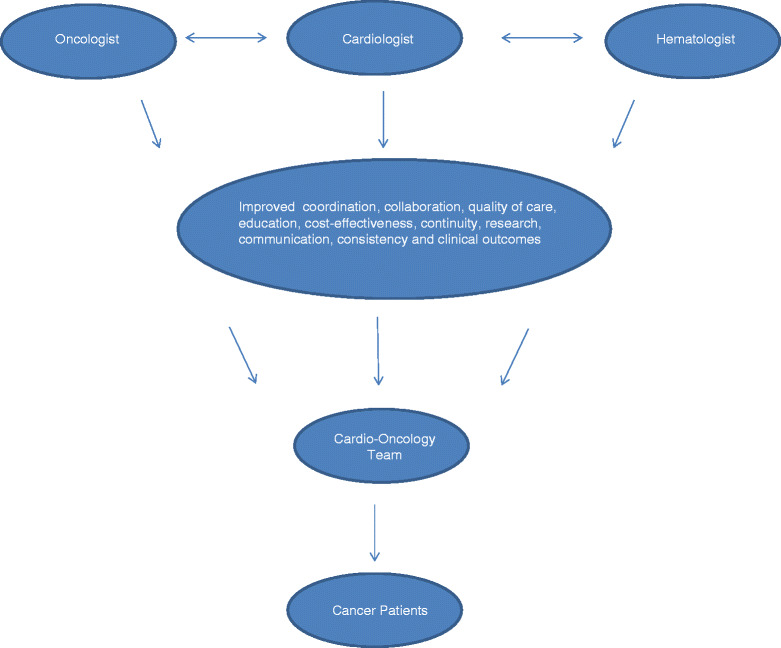
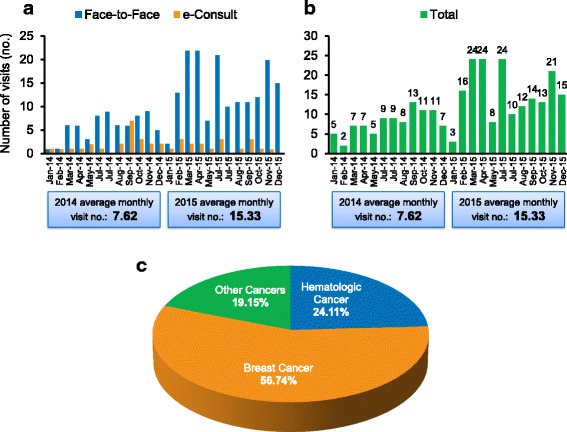
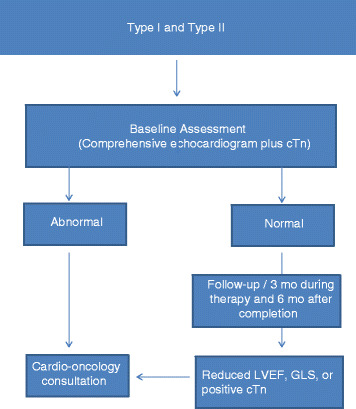
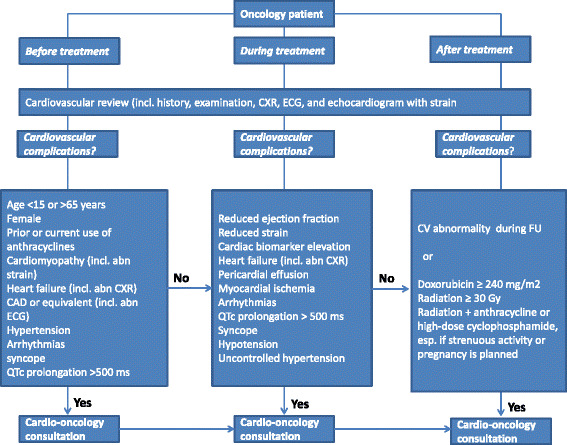
Results: Cardiotoxicity can lead to congestive heart failure and cardiac death. In fact, chemotherapy-related cardiac dysfunction may carry one of the worst prognoses of all types of cardiomyopathies, and has a profound impact on morbidity and mortality in oncology patients. Other complex clinical situations involve cancer patients who might benefit from a highly curative drug in terms of cancer survival but face limitations of its administration because of concomitant cardiovascular diseases. Indeed, the balance between the benefits and risks of the cancer therapy regimen in the context of the cardiovascular status of the individual patient can sometimes be extraordinarily challenging. A subspecialty with a multidisciplinary integrative approach between oncologists, hematologists, cardiologists, among others has thus emerged to address these issues, termed cardio-oncology. Cardio-oncology addresses the spectrum of prevention, detection, monitoring and treatment of cancer patients with cardiovascular diseases, or at risk for cardiotoxicity, in a multidisciplinary manner. In this field, cardiologists assist oncologists and hematologists with cardiovascular recommendations. This can be mediated through e-consultations or face-to-face evaluations.
Conclusion: Cardio-oncology is a subspecialty that assists in the overall care of cancer patients with and without cardiovascular disease in an interdisciplinary fashion. We believe that this partnership of sharing responsibilities and experiences among health-care team members can potentially decrease cancer therapeutics-related cardiovascular complications and improve clinical outcomes.
Keywords: Cardio-oncology; Cardio-oncology program; Cardiotoxicity; Cardiovascular risk factors; Electronic medical records; Multidisciplinary.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources