

Radiotherapy-Immunotherapy Combination: How Will We Bridge the Gap Between Pre-Clinical Promise and Effective Clinical Delivery?
- PMID: 33530329
- PMCID: PMC7865752
- DOI: 10.3390/cancers13030457
Radiotherapy-Immunotherapy Combination: How Will We Bridge the Gap Between Pre-Clinical Promise and Effective Clinical Delivery?
Abstract
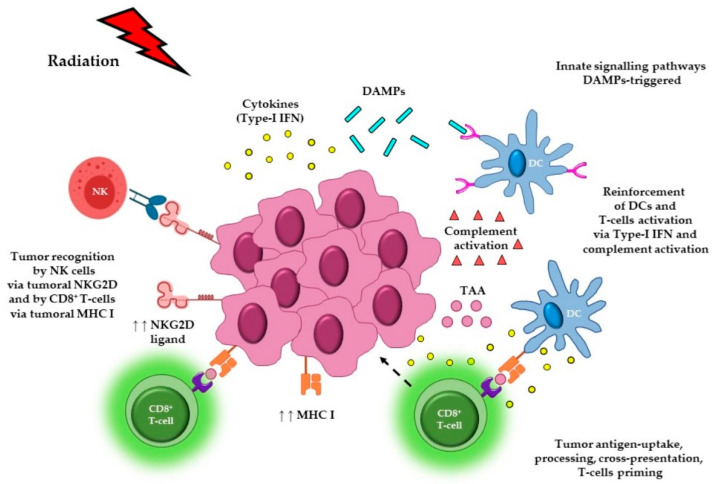
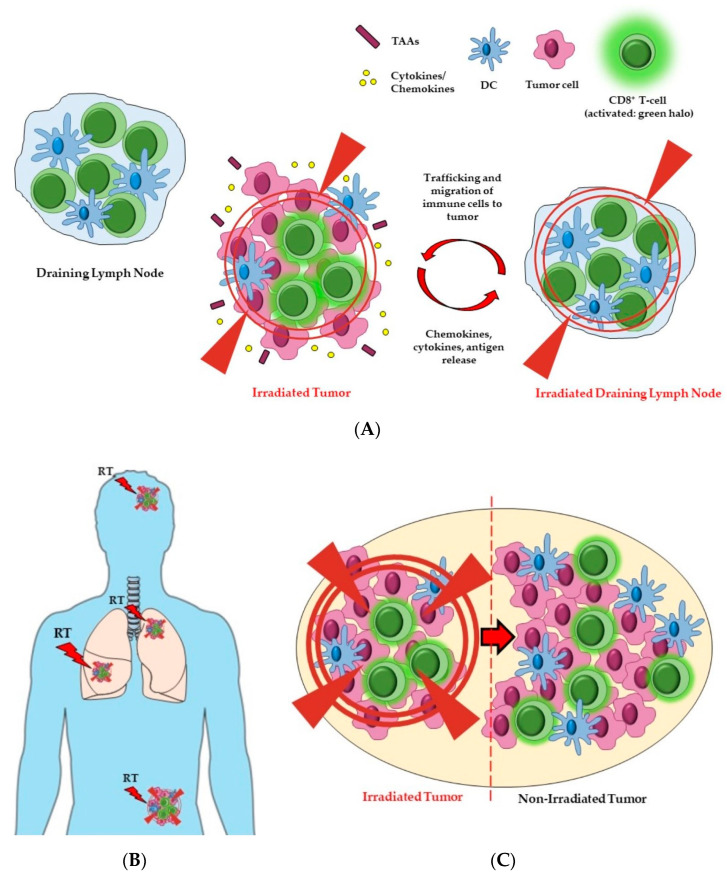
Radiotherapy (RT) is highly effective at directly killing tumor cells and plays an important part in cancer treatments being delivered to around 50% of all cancer patients. The additional immunomodulatory properties of RT have been investigated, and if exploited effectively, have the potential to further improve the efficacy of RT and cancer outcomes. The initial results of combining RT with immunomodulatory agents have generated promising data in pre-clinical studies, which has in turn led to a large number of RT and immunotherapy clinical trials. The overarching aim of these combinations is to enhance anti-tumor immune responses and improve responses rates and patient outcomes. In order to maximize this undoubted opportunity, there remain a number of important questions that need to be addressed, including: (i) the optimal RT dose and fractionation schedule; (ii) the optimal RT target volume; (iii) the optimal immuno-oncology (IO) agent(s) to partner with RT; (iv) the optimal site(s)/route(s) of administration of IO agents; and finally, the optimal RT schedule. In this review, we will summarize progress to date and identify current gaps in knowledge that need to be addressed in order to facilitate effective clinical translation of RT and IO agent combinations.
Keywords: administration sequencing; administration site/route; fractionation schedule; immuno-oncology agents; immunotherapy; radiotherapy; radiotherapy dose; treatment field; tumor volume.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Schoenhals J.E., Skrepnik T., Selek U., Cortez M.A., Li A., Welsh J.W. Optimizing Radiotherapy with Immunotherapeutic Approaches. In: Naing A., Hajjar J., editors. Immunotherapy. 1st ed. Springer; Cham, Switzerland: 2017. pp. 53–71. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
