

Poly(methyl methacrylate) Bone Cement Composite Can Be Refilled with Antibiotics after Implantation in Femur or Soft Tissue
- PMID: 33530542
- PMCID: PMC7838923
- DOI: 10.3390/jfb12010008
Poly(methyl methacrylate) Bone Cement Composite Can Be Refilled with Antibiotics after Implantation in Femur or Soft Tissue
Abstract
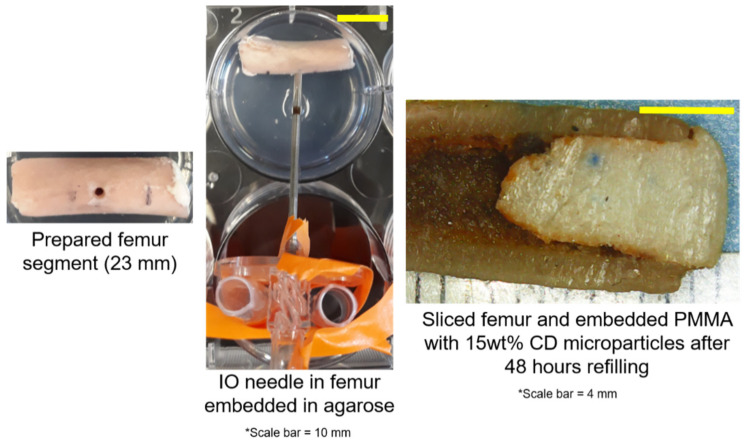
While periprosthetic joint infections (PJIs) result in a small percentage of patients following arthroplasties, they are challenging to treat if they spread into bone and soft tissue. Treatment involves delivering antibiotics using poly(methyl methacrylate) (PMMA) bone cement. However, antibiotic release is insufficient for prolonged infections. Previous work demonstrated efficacy of incorporating insoluble cyclodextrin (CD) microparticles into PMMA to improve antibiotic release and allow for post-implantation drug refilling to occur in a tissue-mimicking model. To simulate how antibiotic refilling may be possible in more physiologically relevant models, this work investigated development of bone and muscle refilling models. The bone refilling model involved embedding PMMA-CD into rabbit femur and administering antibiotic via intraosseous infusion. Muscle tissue refilling model involved implanting PMMA-CD beads in bovine muscle tissue and administering antibiotic via tissue injection. Duration of antimicrobial activity of refilled PMMA-CD was evaluated. PMMA-CD composite in bone and muscle tissue models was capable of being refilled with antibiotics and resulted in prolonged antimicrobial activity. PMMA-CD provided sustained and on-demand antimicrobial activity without removal of implant if infection develops. Intraosseous infusion appeared to be a viable technique to enable refilling of PMMA-CD after implantation in bone, reporting for the first time the ability to refill PMMA in bone.
Keywords: PMMA; antibiotic; bone cement; femur; refill.
Conflict of interest statement
The authors declare no conflict of interest.
Figures










References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
