

Efficacy of Lesion Specific Portals in Endoscopic Treatment of Calcaneal Bone Cyst: A Case Report and Literature Review
- PMID: 33530595
- PMCID: PMC7911473
- DOI: 10.3390/medicina57020111
Efficacy of Lesion Specific Portals in Endoscopic Treatment of Calcaneal Bone Cyst: A Case Report and Literature Review
Abstract
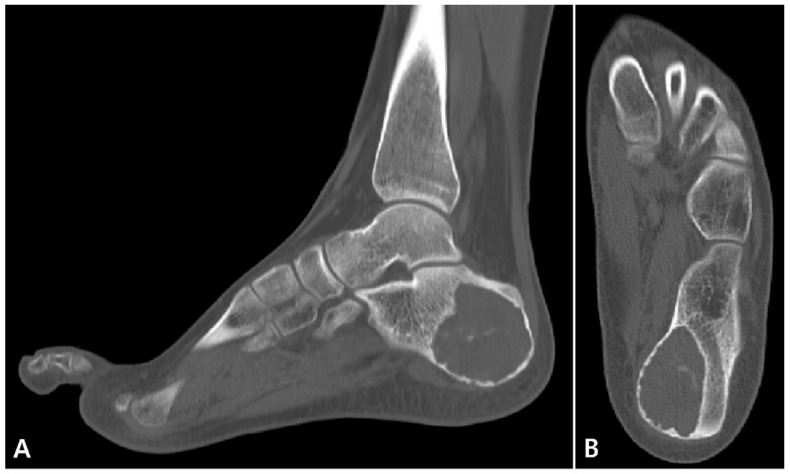
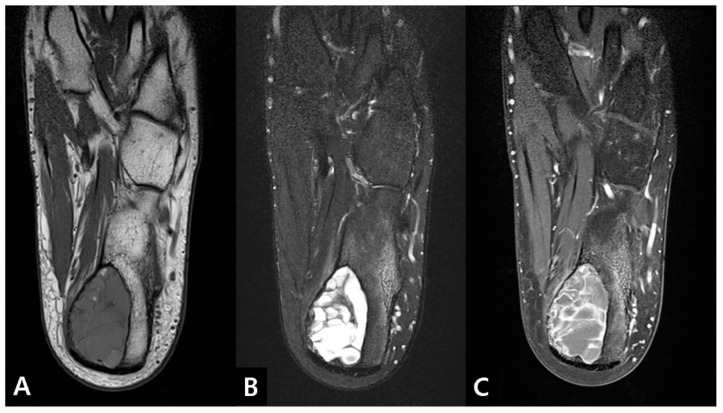
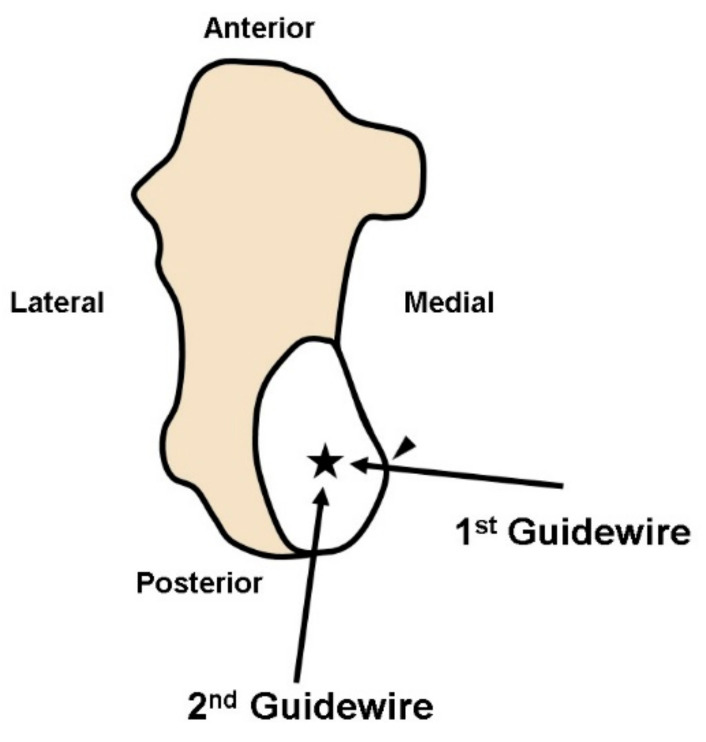
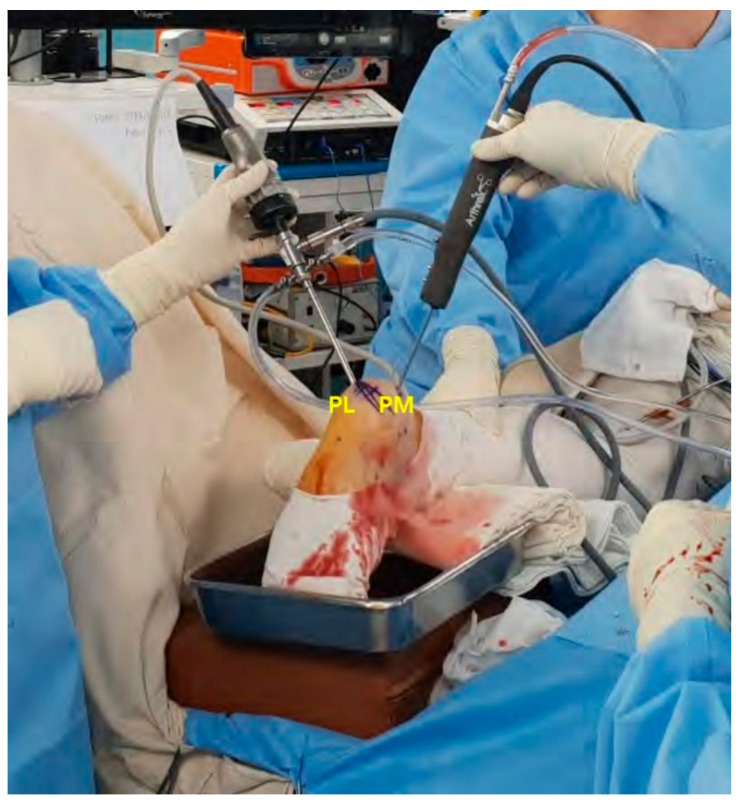
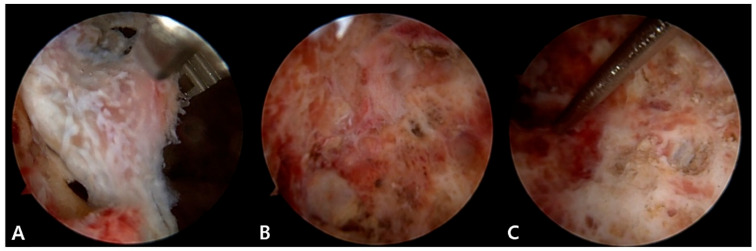
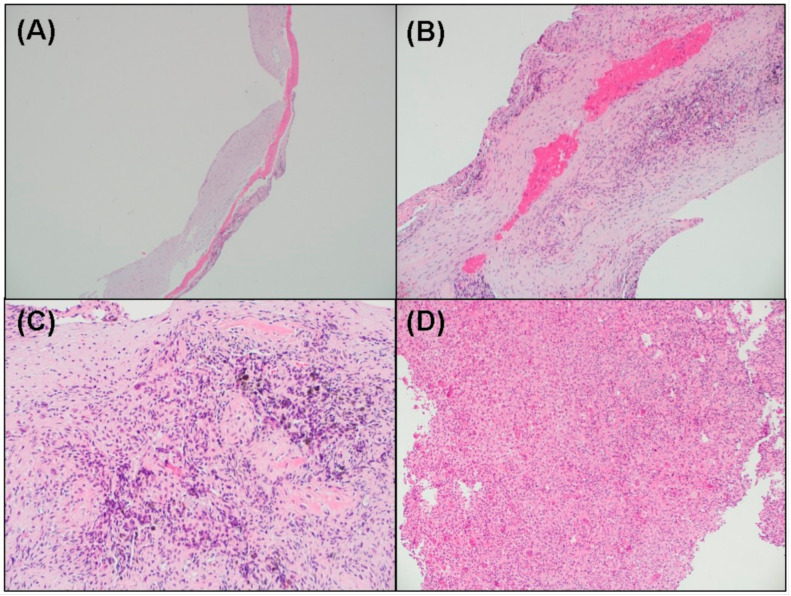
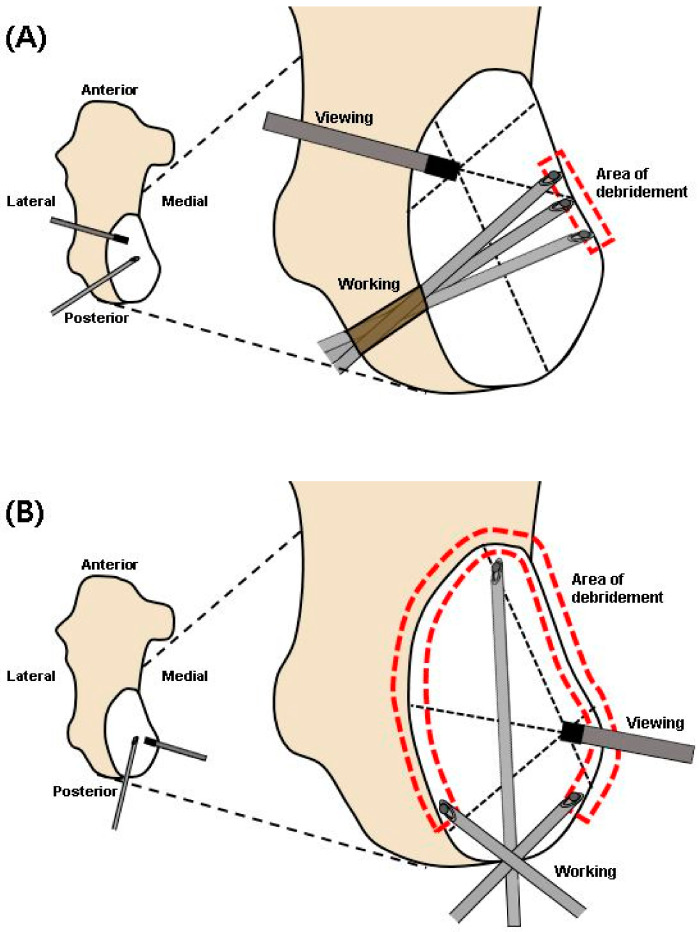
Background: Calcaneal bone cysts rarely occur and most of them are known to be benign. Among them, simple bone cysts (SBCs) third most commonly occur in the calcaneus and of the many surgical treatment options, endoscopic curettage is recently gaining popularity among surgeons due to its advantages of minimal invasiveness and optimal visualization. As for portal placement for endoscopy, two lateral portals are considered a standard technique, but no rationale has been established for SBCs with abnormal geometry. This case report suggests an SBC with secondary aneurysmal change located outside the Ward's triangle, as well as an appropriate endoscopic approach. Case Presentation: An 18-year-old male high school student presented with a main complaint of pain at the hind foot level for the past one year, without significant improvement from conservative treatment. An endoscopic curettage through the lesion specific two posterior portals and bone graft using allogeneic cancellous bone were performed. SBC with a secondary aneurysmal bone cyst was diagnosed on pathology. At a one-year follow-up, the patient was painless and had returned to his regular activities. Physical and radiographic examinations revealed that the lesion was completely healed without any evidence of recurrence. Conclusion: For calcaneal bone cysts located at the posterior aspect of the calcaneus, eccentrically medial and abnormally long anterior-posteriorly, we suggest an endoscopic procedure using lesion specific portals such as two posterior portals.
Keywords: benign bone tumors; calcaneal bone cysts; endoscopic curettage; portal.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures




Similar articles
-
Treatment of a unicameral bone cyst of calcaneus with endoscopic curettage and percutaneous filling with corticocancellous allograft.J Foot Ankle Surg. 2010 Jan-Feb;49(1):93-7. doi: 10.1053/j.jfas.2009.08.005. J Foot Ankle Surg. 2010. PMID: 20123299
-
Endoscopic curettage and allografting of simple bone cysts of the calcaneus in young soccer players: Report of three cases.Foot (Edinb). 2022 May;51:101868. doi: 10.1016/j.foot.2021.101868. Epub 2021 Sep 25. Foot (Edinb). 2022. PMID: 35483303
-
Endoscopic Versus Open Surgery for Calcaneal Bone Cysts: A Preliminary Report.J Foot Ankle Surg. 2016 Jul-Aug;55(4):782-7. doi: 10.1053/j.jfas.2016.03.006. Epub 2016 Apr 8. J Foot Ankle Surg. 2016. PMID: 27067197
-
Unicameral bone cyst of the calcaneus in children.J Pediatr Orthop. 1994 Jan-Feb;14(1):101-4. doi: 10.1097/01241398-199401000-00020. J Pediatr Orthop. 1994. PMID: 8113358 Review.
-
Simple bone cyst of the calcaneus. A case report and literature review.J Am Podiatr Med Assoc. 1994 Mar;84(3):127-30. doi: 10.7547/87507315-84-3-127. J Am Podiatr Med Assoc. 1994. PMID: 8040810 Review.
Cited by
-
Allogenic Cancellous Bone versus Injectable Bone Substitute for Endoscopic Treatment of Simple Bone Cyst and Intraosseous Lipoma of the Calcaneus and Is Intraosseous Lipoma a Developmental Stage of a Simple Bone Cyst?J Clin Med. 2023 Jun 26;12(13):4272. doi: 10.3390/jcm12134272. J Clin Med. 2023. PMID: 37445307 Free PMC article.
References
-
- Dormans J., Pill S. Fractures through bone cysts: Unicameral bone cysts, aneurysmal bone cysts, fibrous cortical defects, and nonossifying fibromas. Instr. Course Lect. 2002;51:457–467. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
