

Brain-Computer Interfaces for Communication: Preferences of Individuals With Locked-in Syndrome
- PMID: 33530868
- PMCID: PMC7934157
- DOI: 10.1177/1545968321989331
Brain-Computer Interfaces for Communication: Preferences of Individuals With Locked-in Syndrome
Abstract
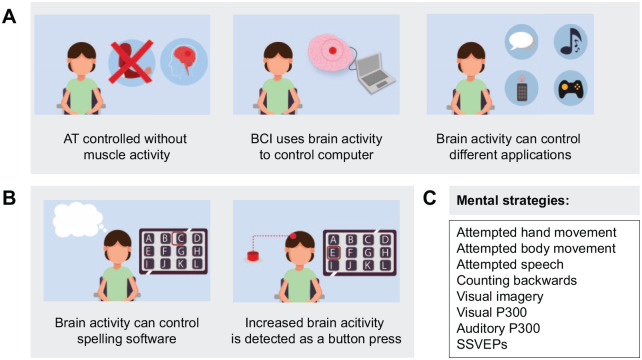
Background: Brain-computer interfaces (BCIs) have been proposed as an assistive technology (AT) allowing people with locked-in syndrome (LIS) to use neural signals to communicate. To design a communication BCI (cBCI) that is fully accepted by the users, their opinion should be taken into consideration during the research and development process.
Objective: We assessed the preferences of prospective cBCI users regarding (1) the applications they would like to control with a cBCI, (2) the mental strategies they would prefer to use to control the cBCI, and (3) when during their clinical trajectory they would like to be informed about AT and cBCIs. Furthermore, we investigated if individuals diagnosed with progressive and sudden onset (SO) disorders differ in their opinion.
Methods: We interviewed 28 Dutch individuals with LIS during a 3-hour home visit using multiple-choice, ranking, and open questions. During the interview, participants were informed about BCIs and the possible mental strategies.
Results: Participants rated (in)direct forms of communication, computer use, and environmental control as the most desired cBCI applications. In addition, active cBCI control strategies were preferred over reactive strategies. Furthermore, individuals with progressive and SO disorders preferred to be informed about AT and cBCIs at the moment they would need it.
Conclusions: We show that individuals diagnosed with progressive and SO disorders preferred, in general, the same applications, mental strategies, and time of information. By collecting the opinion of a large sample of individuals with LIS, this study provides valuable information to stakeholders in cBCI and other AT development.
Keywords: brain-computer interface; communication; locked-in syndrome; opinion; user-centered design.
Conflict of interest statement
Figures





References
-
- Recommendations for use of uniform nomenclature pertinent to patients with severe alterations in consciousness. American Congress of Rehabilitation Medicine. Arch Phys Med Rehabil. 1995;76:205-209. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
