

Comparable results using 2.0-mm vs. 3.5-mm screw augmentation in midshaft clavicle fractures: a 10-year experience
- PMID: 33531034
- PMCID: PMC7851941
- DOI: 10.1186/s40001-021-00487-w
Comparable results using 2.0-mm vs. 3.5-mm screw augmentation in midshaft clavicle fractures: a 10-year experience
Abstract
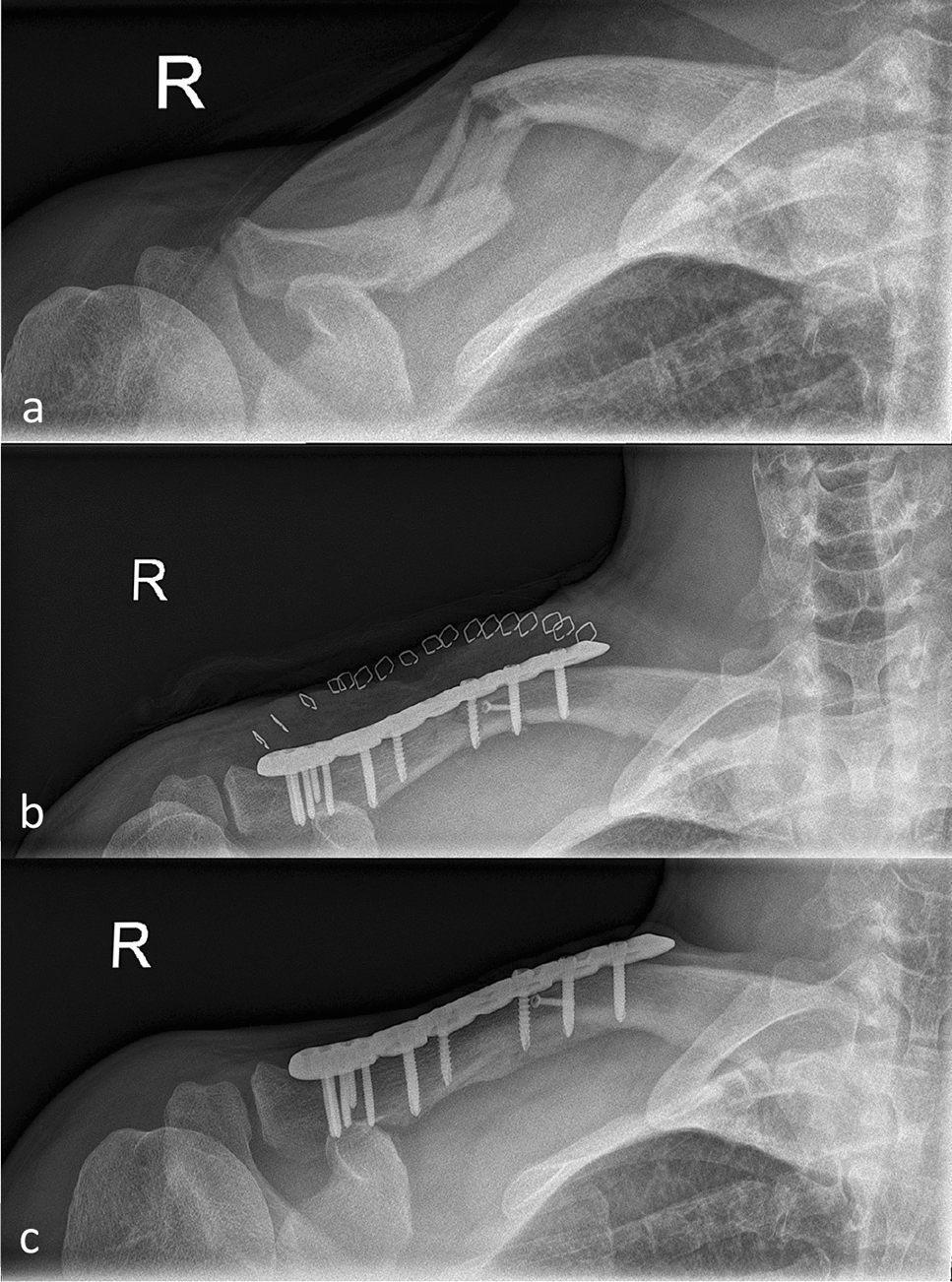
Purpose: Absence of cortical alignment in wedge-shaped and multifragmentary fractures (Fx) results in decreased fixation stability. The aim of this study was to compare the outcome using 2.0- vs. 3.5-mm screws for open reduction and internal fixation (ORIF) in dislocated, wedge-shaped or fragmentary midshaft clavicle fractures.
Materials and methods: Patients suffering from AO/OTA 15 2.A-C midshaft clavicle fractures were operatively treated between 2008 and 2018. 2.0- or 3.5-mm cortical screws were used to restore anatomic alignment in dislocated, wedge-shaped and fragmentary clavicle fractures. Data of radiologic outcome were collected until fracture consolidation was identified.
Results: 80 consecutive patients with a mean age of 44.5 ± 16.3 years, who were operatively treated for dislocated midshaft clavicle fractures were enrolled. 40 patients were treated using 2.0-mm and 40 patients using routine 3.5-mm cortical screws, respectively. Time to fracture consolidation was 12.8 ± 7.8 months. No mal- or non-unions occurred during routine follow-up until 18 months postoperatively.
Conclusion: Restoring anatomic alignment in wedge or fragmentary clavicle fractures can ultimately be addressed using cortical screw augmentation. Both groups showed comparable results with respect to fracture reduction, fixation and stability as well as time to consolidation of the fracture, while the 2.0-mm screw diameter was associated with easier handling of small Fx fragments.
Keywords: Alignment; Clavicle; Cortical; Fracture; Osteosynthesis; Plate; Screw.
Conflict of interest statement
None of the authors declares any conflict of interest.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
