

Central serous chorioretinopathy in active endogenous Cushing's syndrome
- PMID: 33531597
- PMCID: PMC7854641
- DOI: 10.1038/s41598-021-82536-2
Central serous chorioretinopathy in active endogenous Cushing's syndrome
Abstract
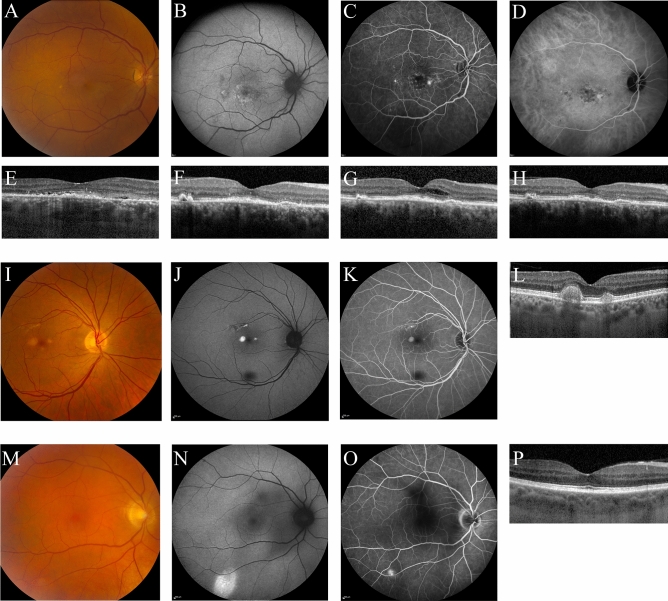
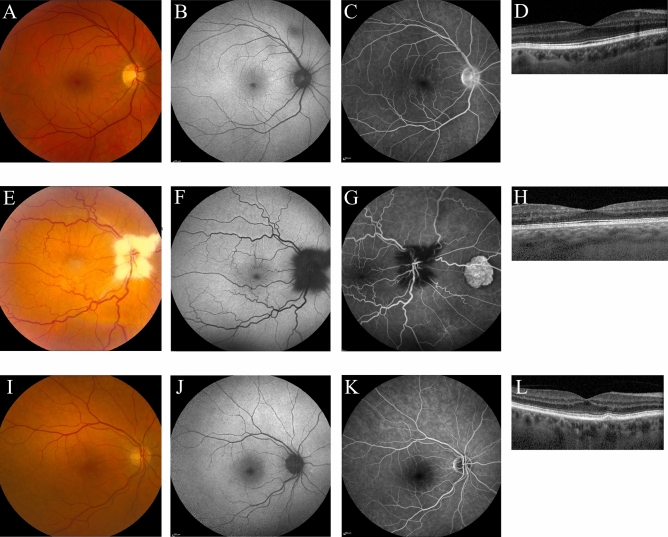
Multiple case series have provided evidence for a relatively high incidence of central serous chorioretinopathy (CSC) in patients with active Cushing's syndrome (CS). We describe the ophthalmological status in detail of consecutive patients with active endogenous CS (either de novo or recurrent active endogenous CS) in this prospective cohort study. All patients underwent complete ophthalmological examination, including multimodal imaging, which was performed shortly after establishing the diagnosis of active CS in hypercortisolemic state. Eleven CS patients (4 men, 7 women) with active hypercortisolism were included. Abnormalities reminiscent of (subclinical) CSC were found in 3 patients. Optical coherence tomography (OCT) revealed macular subretinal fluid in 1 patient, who was diagnosed as having active CSC and was successfully treated with half-dose photodynamic therapy. Two other patients showed CSC-like abnormalities: an unilateral pseudovitelliform lesion on OCT and hyperfluorescent changes on fluorescein angiography in one patient, and unilateral leakage on fluorescein angiography in the other patient. Mean subfoveal choroidal thickness on enhanced depth imaging OCT was 270 ± 40 μm (range, 178 - 357 μm). Retinal abnormalities resembling (subclinical) CSC may be more common than previously thought in patients with active CS, and may exist even in patients without visual complaints. Clinicians should have a low threshold for ophthalmological evaluation in case of a CS patient with visual symptoms since there may be therapeutic opportunities to prevent vision loss.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
