

Minimally Invasive Modified Lemaire Tenodesis
- PMID: 33532204
- PMCID: PMC7823058
- DOI: 10.1016/j.eats.2020.09.006
Minimally Invasive Modified Lemaire Tenodesis
Abstract
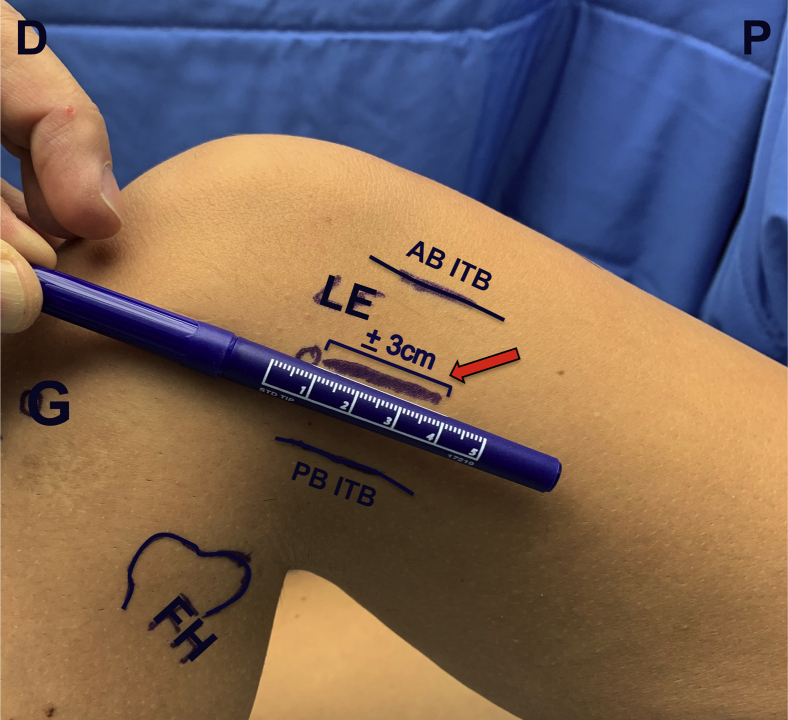
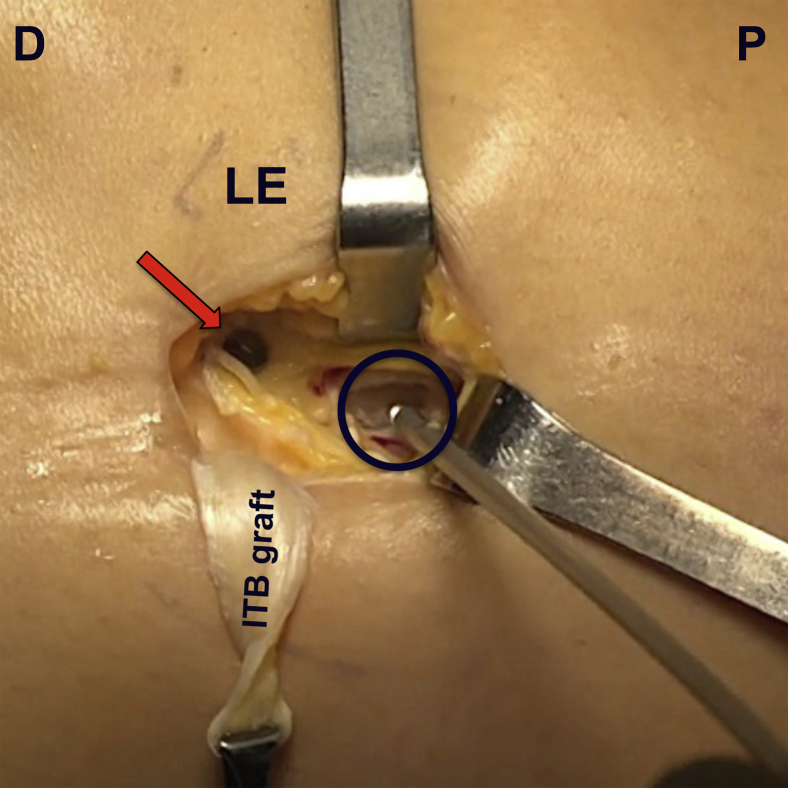
Increasing emphasis in the literature is recently being put on controlling rotational stability in patients with an anterior cruciate ligament rupture by addressing the anterolateral complex during anterior cruciate ligament reconstruction. Many different techniques for lateral extra-articular tenodesis have been described, with the (modified) Lemaire technique being widely favored. Recent literature does report that lateral extra-articular tenodesis leads to a reduction in persistent rotatory laxity and graft rupture rate, but also may be associated with increased pain, reduced quadriceps strength, reduced subjective functional recovery, and cosmetic complaints. Thus this article aims to describe our minimally invasive technique for a modified Lemaire tenodesis.
© 2020 by the Arthroscopy Association of North America. Published by Elsevier.
Figures












References
-
- Segond P. Recherches cliniques et expérimentales sur les épanchements sanguins du genou par entorse. Prog Méd. 1879;16:297–421.
-
- Hess T., Rupp S., Hopf T., Gleitz M.L.J. Lateral tibial avulsion fractures and disruptions to the anterior cruciate ligament: A clinical study of their incidence and correlation. Clin Orthop Relat Res. 1994;303:193–197. - PubMed
-
- Goldman A.B., Pavlov H., Rubenstein D. The Segond fracture of the proximal tibia: A small avulsion that reflects major ligamentous damage. Am J Roentgenol. 1988;151:1163–1167. - PubMed
-
- Musahl V., Rahnemai-Azar A.A., Costello J. The influence of meniscal and anterolateral capsular injury on knee laxity in patients with anterior cruciate ligament injuries. Am J Sports Med. 2016;44:3126–3131. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
