

The DIAMORFOSIS (DIAgnosis and Management Of lung canceR and FibrOSIS) survey: international survey and call for consensus
- PMID: 33532484
- PMCID: PMC7837280
- DOI: 10.1183/23120541.00529-2020
The DIAMORFOSIS (DIAgnosis and Management Of lung canceR and FibrOSIS) survey: international survey and call for consensus
Abstract
Background: Currently there is major lack of agreement on the diagnostic and therapeutic management of patients with idiopathic pulmonary fibrosis (IPF) and lung cancer. Our aim was to identify variations in diagnostic and management strategies across different institutions and provide rationale for a consensus statement on this issue.
Methods: This was a joint-survey by European Respiratory Society (ERS) Assemblies 8, 11 and 12. The survey consisted of 25 questions.
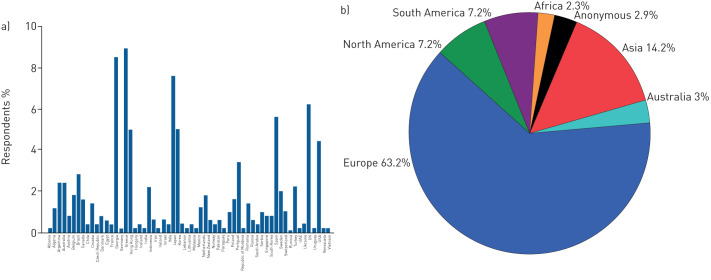
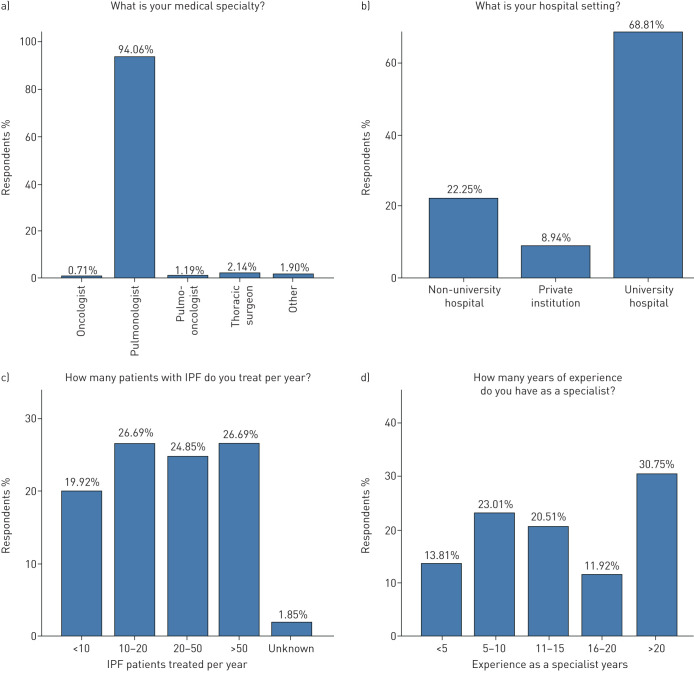
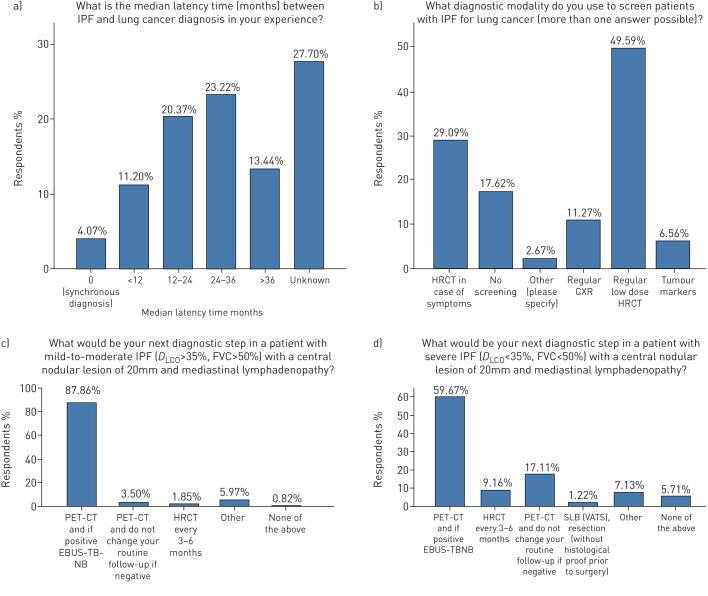
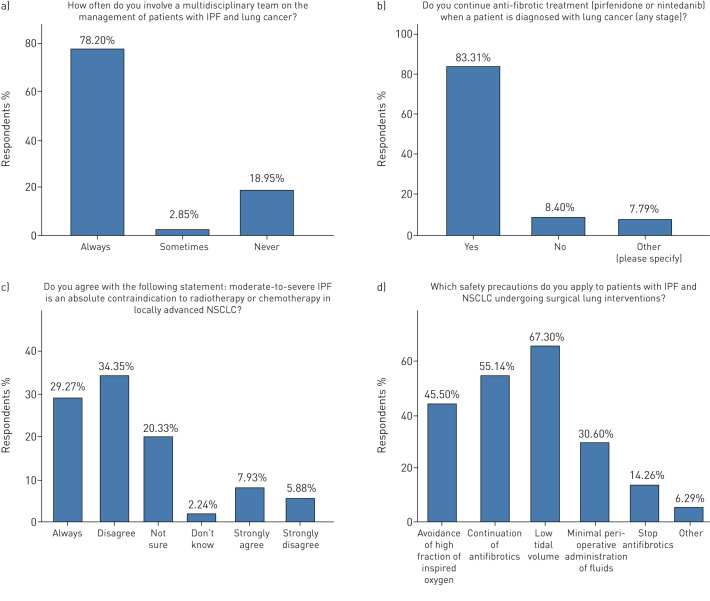
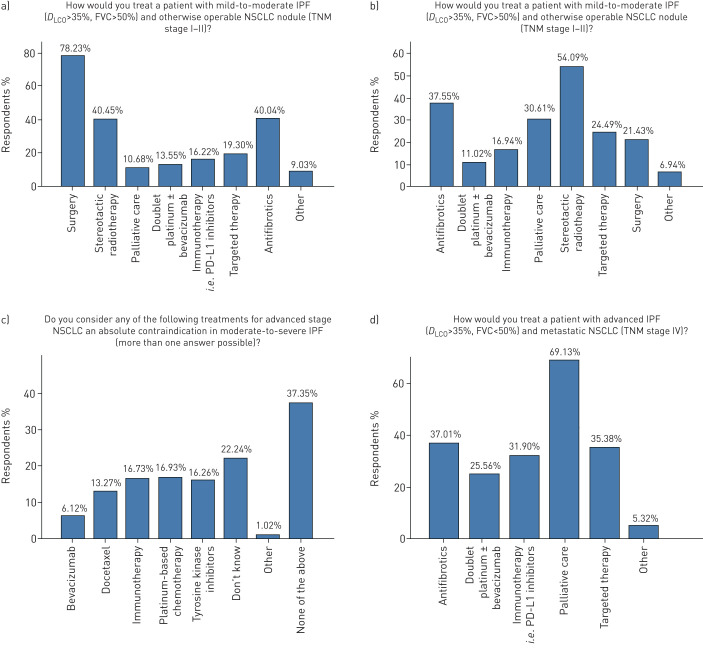
Results: Four hundred and ninety-four (n=494) physicians from 68 different countries and five continents responded to the survey. Ninety-four per cent of participants were pulmonologists, 1.8% thoracic surgeons and 1.9% oncologists; 97.7% were involved in multidisciplinary team approaches on diagnosis and management. Regular low-dose high-resolution computed tomography (HRCT) scan was used by 49.5% of the respondents to screen for lung cancer in IPF. Positron emission tomography (PET) scan and endobronchial ultrasound (EBUS) is performed by 60% and 88% to diagnose nodular lesions with mediastinal lymphadenopathy in patients with advanced and mild IPF, respectively. Eighty-three per cent of respondents continue anti-fibrotics following lung cancer diagnosis; safety precautions during surgical interventions including low tidal volume are applied by 67%. Stereotactic radiotherapy is used to treat patients with advanced IPF (diffusing capacity of the lung for carbon monoxide (D LCO) <35%) and otherwise operable nonsmall cell lung cancer (NSCLC) by 54% of respondents and doublet platinum regimens and immunotherapy for metastatic disease by 25% and 31.9%, respectively. Almost all participants (93%) replied that a consensus statement for the management of these patients is highly warranted.
Conclusion: The diagnosis and management of IPF-lung cancer (LC) is heterogeneous with most respondents calling for a consensus statement.
Copyright ©ERS 2021.
Conflict of interest statement
Conflict of interest: A. Tzouvelekis has received travel grants and consultation fees from Boehringer Ingelheim and Hoffmann La Roche outside the submitted work. Conflict of interest: K. Antoniou has received travel grants and consultation fees from Boehringer Ingelheim and Hoffmann La Roche. Conflict of interest: M. Kreuter has nothing to disclose. Conflict of interest: M. Evison has nothing to disclose. Conflict of interest: T.G. Blum has nothing to disclose. Conflict of interest: V. Poletti has nothing to disclose. Conflict of interest: B. Grigoriu has nothing to disclose. Conflict of interest: C. Vancheri has received unrestricted grants, and speaker and advisory board fees from Boehringer Ingelheim and F. Hoffmann-La Roche Ltd. Conflict of interest: P. Spagnolo reports grants, personal fees and nonfinancial support from Roche, PPM Services and Boehringer-Ingelheim, and reports personal fees from Red X Pharma, Galapagos and Chiesi, outside of the submitted work. Conflict of interest: T. Karampitsakos has nothing to disclose. Conflict of interest: F. Bonella has received travel grants and consultation fees from Boehringer Ingelheim, Hoffmann La Roche, Galapalagos, Savara and BMS. Conflict of interest: A. Wells has received travel grants and consultation fees from Boehringer Ingelheim and Hoffmann La Roche. Conflict of interest: G. Raghu has nothing to disclose. Conflict of interest: M. Molina-Molina reports grants and payment for scientific advice for Roche, Boehringer Ingelheim, Esteve-Teijin, Chiesi, Pfizer, GSK and Galapagos. Conflict of interest: D. Culver has nothing to disclose. Conflict of interest: E. Bendstrup has nothing to disclose. Conflict of interest: N. Mogulkoc has nothing to disclose. Conflict of interest: S. Elia has nothing to disclose. Conflict of interest: J. Cadranel reports grants from BI, and personal fees for consultancy and experts boards from Roche and BI, outside the submitted work. Conflict of interest: D. Bouros reports grants, personal fees, nonfinancial support and other support from BI Hellas, and other support from Roche, outside the submitted work.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous