

Multicenter randomized phase II trial of prophylactic right-half dissection of superior mesenteric artery nerve plexus in pancreatoduodenectomy for pancreatic head cancer
- PMID: 33532687
- PMCID: PMC7832966
- DOI: 10.1002/ags3.12399
Multicenter randomized phase II trial of prophylactic right-half dissection of superior mesenteric artery nerve plexus in pancreatoduodenectomy for pancreatic head cancer
Abstract
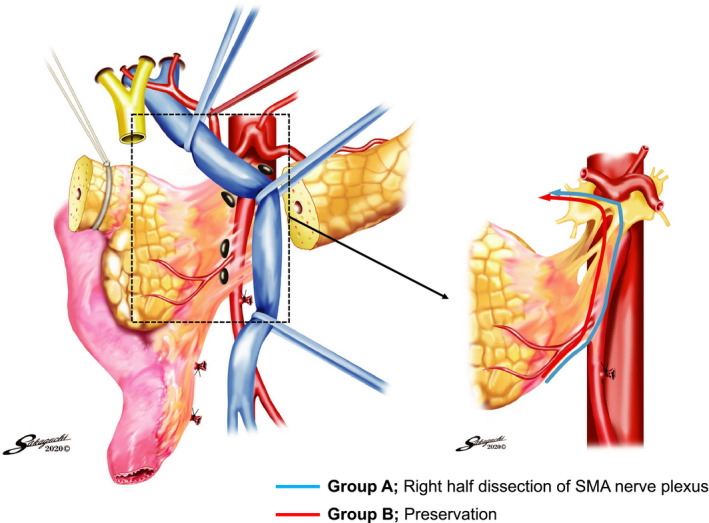
Aim: Right-half dissection of the superior mesenteric artery (SMA) nerve plexus in pancreatoduodenectomy for pancreatic cancer was initiated to accomplish R0 resection; however, subsequent refractory diarrhea was a major concern. This study aimed to evaluate the necessity of this technique.
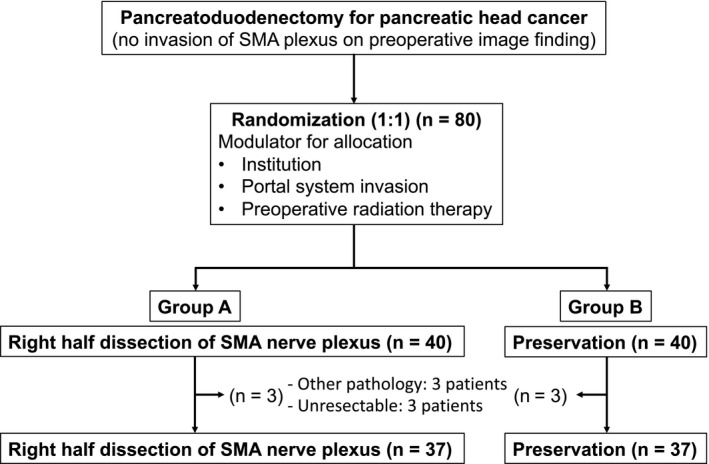
Methods: From April 2014 to June 2018, 74 patients with pancreatic head cancer were randomly allocated to either Group A, in which right-half dissection of the SMA nerve plexus was performed (n = 37), or Group B, in which total preservation of the nerve plexus was performed (n = 37). Short-term, long-term, and survival outcomes were prospectively compared between the groups.
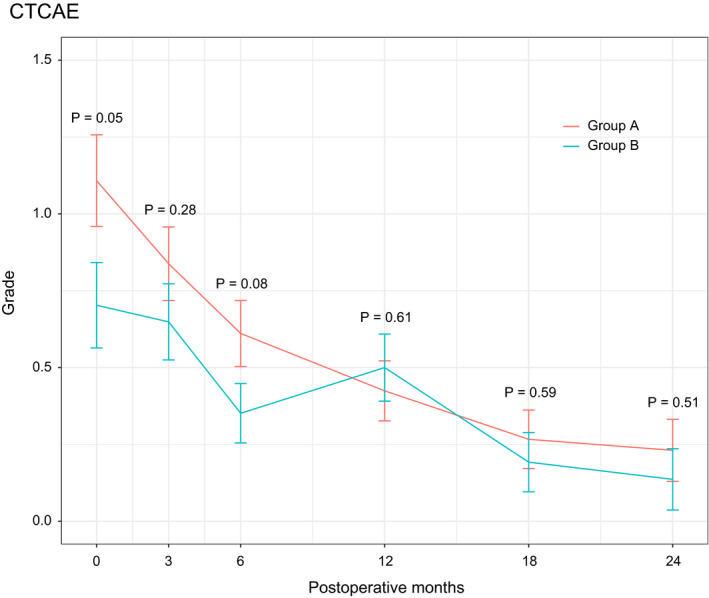
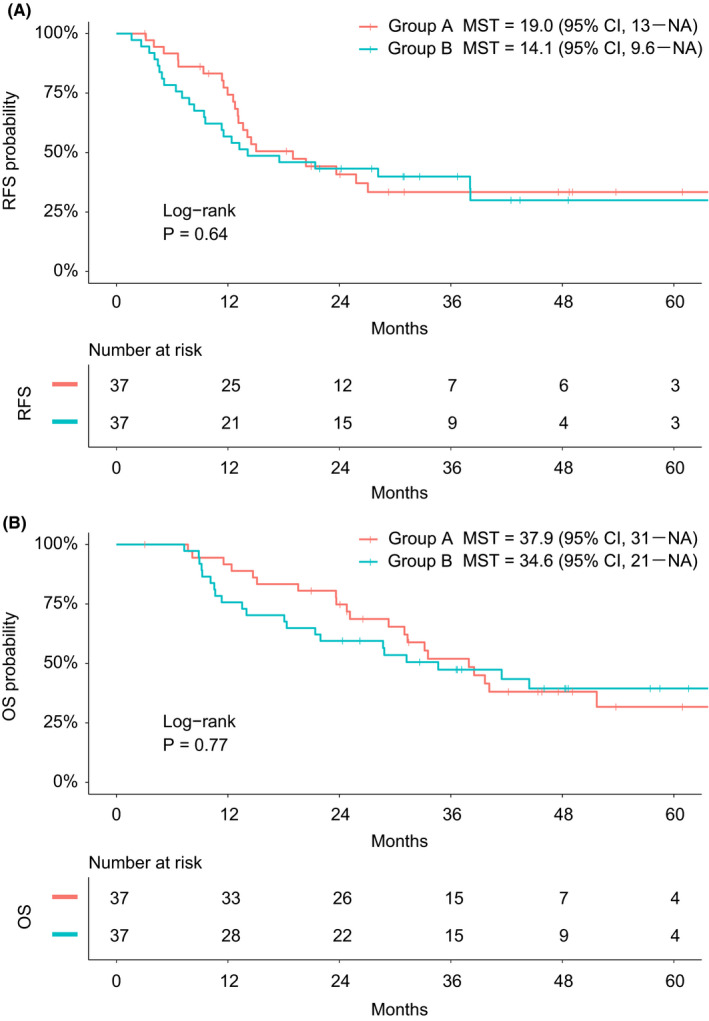
Results: The patient demographics, including the R0 resection rate, were not significantly different between the groups. Postoperative diarrhea occurred in 26 (70.3%) patients in Group A and 18 (48.6%) patients in Group B. There was a tendency for the development of severe diarrhea in Group A within 1 year postoperatively, and the frequency of diarrhea gradually decreased within 2 years, although that did not affect tolerance to adjuvant chemotherapy. There was no difference in either locoregional recurrence (27.0% vs 32.4%) or systemic recurrence (46.0% vs 46.0%). The median overall survival time in Groups A and B was 37.9 and 34.6 months, respectively (P = 0.77).
Conclusion: We did not demonstrate a clinical impact of right-half dissection of the SMA nerve plexus on locoregional recurrence or survival. Therefore, the prophylactic dissection of the SMA nerve plexus is unnecessary given that refractory diarrhea could be induced by this technique (UMIN000012241).
Keywords: pancreatic head cancer; pancreatoduodenectomy; phase II trial; superior mesenteric artery nerve plexus.
© 2020 The Authors. Annals of Gastroenterological Surgery published by John Wiley & Sons Australia, Ltd on behalf of The Japanese Society of Gastroenterology.
Conflict of interest statement
Conflict of Interest: The authors have no commercial affiliations that can pose any conflicts of interest in connection with this study. Funding: No funding was received for this study.
Figures
References
-
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74(11):2913–21. - PubMed
-
- Egawa S, Toma H, Ohigashi H, Okusaka T, Nakao A, Hatori T, et al. Japan Pancreatic Cancer Registry; 30th year anniversary: Japan Pancreas Society. Pancreas. 2012;41(7):985–92. - PubMed
-
- Pedrazzoli S, DiCarlo V, Dionigi R, Mosca F, Pederzoli P, Pasquali C, et al. Standard versus extended lymphadenectomy associated with pancreatoduodenectomy in the surgical treatment of adenocarcinoma of the head of the pancreas: a multicenter, prospective, randomized study. Lymphadenectomy Study Group. Ann Surg. 1998;228(4):508–17. - PMC - PubMed
-
- Yeo CJ, Cameron JL, Sohn TA, Coleman JoAnn, Sauter PK, Hruban RH, et al. Pancreaticoduodenectomy with or without extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma: comparison of morbidity and mortality and short‐term outcome. Ann Surg. 1999;229(5):613–22; discussion 22–4. - PMC - PubMed
-
- Farnell MB, Pearson RK, Sarr MG, DiMagno EP, Burgart LJ, Dahl TR, et al. A prospective randomized trial comparing standard pancreatoduodenectomy with pancreatoduodenectomy with extended lymphadenectomy in resectable pancreatic head adenocarcinoma. Surgery. 2005;138(4):618–28; discussion 28–30. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
