

This is a preprint.
Mapping a Pandemic: SARS-CoV-2 Seropositivity in the United States
- PMID: 33532807
- PMCID: PMC7852277
- DOI: 10.1101/2021.01.27.21250570
Mapping a Pandemic: SARS-CoV-2 Seropositivity in the United States
Update in
-
Undiagnosed SARS-CoV-2 seropositivity during the first 6 months of the COVID-19 pandemic in the United States.Sci Transl Med. 2021 Jul 7;13(601):eabh3826. doi: 10.1126/scitranslmed.abh3826. Epub 2021 Jun 22. Sci Transl Med. 2021. PMID: 34158410 Free PMC article.
Abstract
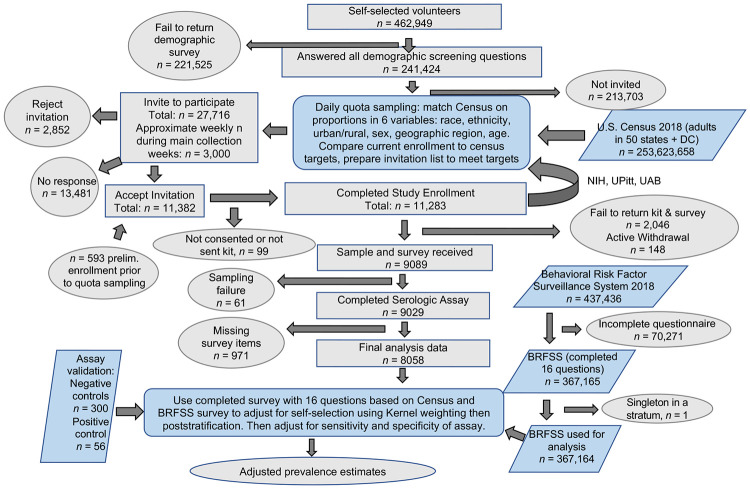
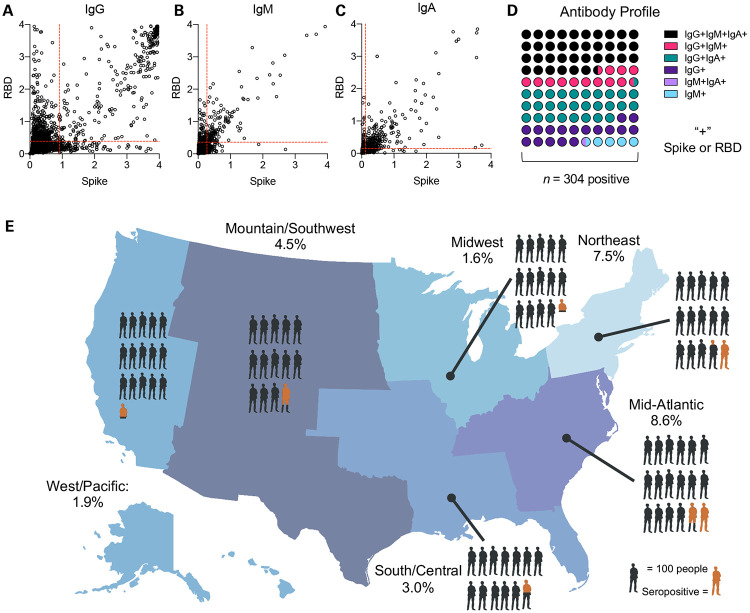
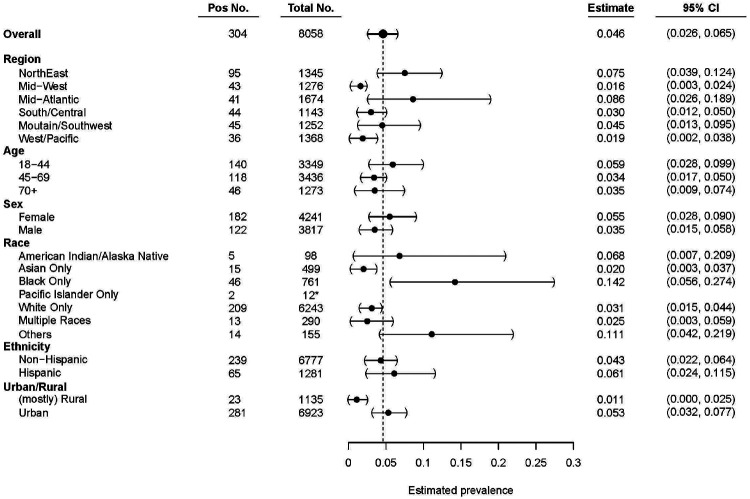
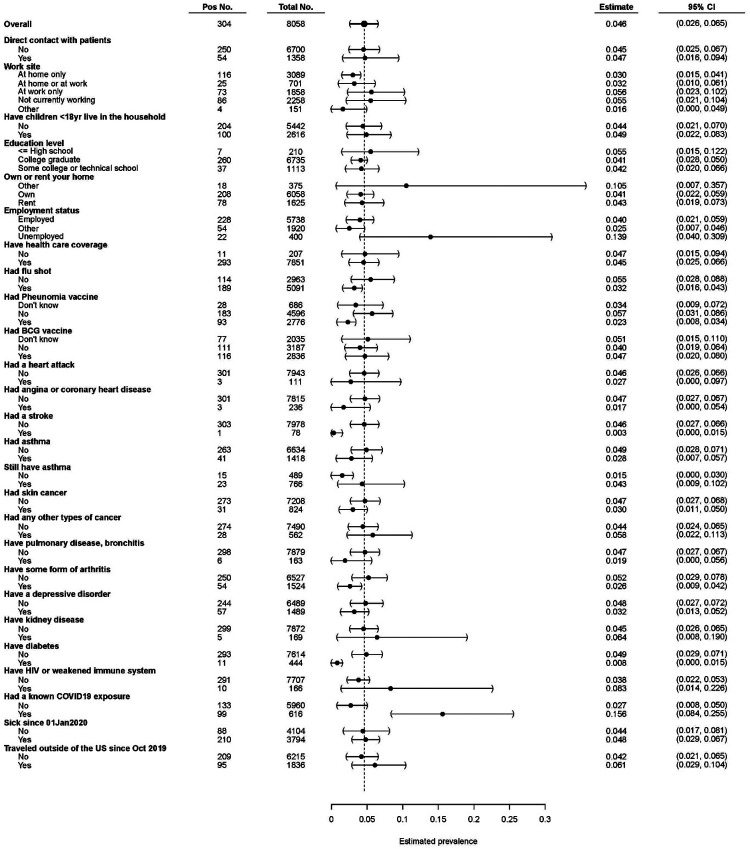
Asymptomatic SARS-CoV-2 infection and delayed implementation of diagnostics have led to poorly defined viral prevalence rates. To address this, we analyzed seropositivity in US adults who have not previously been diagnosed with COVID-19. Individuals with characteristics that reflect the US population (n = 11,382) and who had not previously been diagnosed with COVID-19 were selected by quota sampling from 241,424 volunteers (ClinicalTrials.gov NCT04334954). Enrolled participants provided medical, geographic, demographic, and socioeconomic information and 9,028 blood samples. The majority (88.7%) of samples were collected between May 10th and July 31st, 2020. Samples were analyzed via ELISA for anti-Spike and anti-RBD antibodies. Estimation of seroprevalence was performed by using a weighted analysis to reflect the US population. We detected an undiagnosed seropositivity rate of 4.6% (95% CI: 2.6 - 6.5%). There was distinct regional variability, with heightened seropositivity in locations of early outbreaks. Subgroup analysis demonstrated that the highest estimated undiagnosed seropositivity within groups was detected in younger participants (ages 18-45, 5.9%), females (5.5%), Black/African American (14.2%), Hispanic (6.1%), and Urban residents (5.3%), and lower undiagnosed seropositivity in those with chronic diseases. During the first wave of infection over the spring/summer of 2020 an estimate of 4.6% of adults had a prior undiagnosed SARS-CoV-2 infection. These data indicate that there were 4.8 (95% CI: 2.8-6.8) undiagnosed cases for every diagnosed case of COVID-19 during this same time period in the United States, and an estimated 16.8 million undiagnosed cases by mid-July 2020.
Figures
References
-
- Long Q-X, Liu B-Z, Deng H-J, et al. Antibody responses to SARS-CoV-2 in patients with COVID-19. Nature medicine. 2020:1–4. - PubMed
Publication types
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous