

Neurosurgical experience of managing optic pathway gliomas
- PMID: 33532921
- PMCID: PMC8184710
- DOI: 10.1007/s00381-021-05060-8
Neurosurgical experience of managing optic pathway gliomas
Abstract
Background: Optic pathway gliomas (OPGs), also known as visual pathway gliomas, are debilitating tumors that account for 3-5% of all pediatric brain tumors. They are most commonly WHO grade 1 pilocytic astrocytomas and frequently occur in patients with neurofibromatosis type 1. The location of these tumors results in visual loss and blindness, endocrine and hypothalamic dysfunction, hydrocephalus, and premature death. Their involvement of the visual pathways and proximity to other eloquent brain structures typically precludes complete resection or optimal radiation dosing without incurring significant neurological injury. There are various surgical interventions that can be performed in relation to these lesions including biopsy, cerebrospinal fluid diversion, and partial or radical resection, but their role is a source of debate. This study catalogues our surgical experience and patient outcomes in order to support decision-making in this challenging pathology.
Methods: A retrospective review of all cases of OPGs treated in a single center from July 1990 to July 2020. Data was collected on patient demographics, radiographic findings, pathology, and management including surgical interventions. Outcome data included survival, visual function, endocrine, and hypothalamic dysfunction.
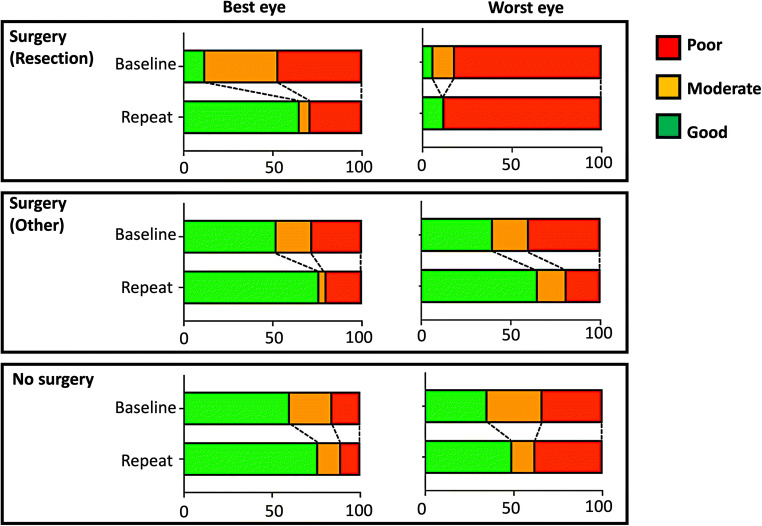
Results: One hundred twenty-one patients with OPG were identified, and 50 of these patients underwent a total of 104 surgical procedures. These included biopsy (31), subtotal or gross total resection (20 operations in 17 patients), cyst drainage (17), Ommaya reservoir insertion (9), or cerebrospinal fluid diversion (27). During the study period, there was 6% overall mortality, 18% hypothalamic dysfunction, 20% endocrine dysfunction, and 42% had some cognitive dysfunction. At diagnosis 75% of patients had good or moderate visual function in at least one eye, and overall, this improved to 83% at the end of the study period. In comparison the worst eye had good or moderate visual function in 56%, and this reduced to 53%. Baseline and final visual function were poorer in patients who had a surgical resection, but improvements in vision were still found-particularly in the best eye.
Discussion/conclusion: OPG are debilitating childhood tumor that have lifelong consequences in terms of visual function and endocrinopathies/hypothalamic dysfunction; this can result in substantial patient morbidity. Decisions regarding management and the role of surgery in this condition are challenging and include cerebrospinal fluid diversion, biopsy, and in highly select cases cystic decompression or surgical resection. In this paper, we review our own experience, outcomes, and surgical philosophy.
Keywords: Glioma; Management; Optic; Pathway; Visual.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
-
- Binning MJ, Liu JK, Kestle JRW, Brockmeyer DL, Walker ML. Optic pathway gliomas: a review. Neurosurg Focus. 2007;23:E2. - PubMed
-
- Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, Ohgaki H, Wiestler OD, Kleihues P, Ellison DW. The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol. 2016;131:803–820. - PubMed
-
- Helfferich J, Nijmeijer R, Brouwer OF et al. Neurofibromatosis type 1 associated low grade gliomas: a comparison with sporadic low grade gliomas. Crit Rev Oncol Hematol. 2016;104:30–41. - PubMed
-
- Jacob K, Albrecht S, Sollier C, Faury D, Sader E, Montpetit A, Serre D, Hauser P, Garami M, Bognar L, Hanzely Z, Montes JL, Atkinson J, Farmer JP, Bouffet E, Hawkins C, Tabori U, Jabado N. Duplication of 7q34 is specific to juvenile pilocytic astrocytomas and a hallmark of cerebellar and optic pathway tumours. Br J Cancer. 2009;101:722–733. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
