

Evaluating the Effectiveness of Diabetes Shared Medical Appointments (SMAs) as Implemented in Five Veterans Affairs Health Systems: a Multi-site Cluster Randomized Pragmatic Trial
- PMID: 33532956
- PMCID: PMC8175536
- DOI: 10.1007/s11606-020-06570-y
Evaluating the Effectiveness of Diabetes Shared Medical Appointments (SMAs) as Implemented in Five Veterans Affairs Health Systems: a Multi-site Cluster Randomized Pragmatic Trial
Abstract
Objective: To examine whether diabetes shared medical appointments (SMAs) implemented as part of usual clinical practice in diverse health systems are more effective than usual care in improving and sustaining A1c improvements.
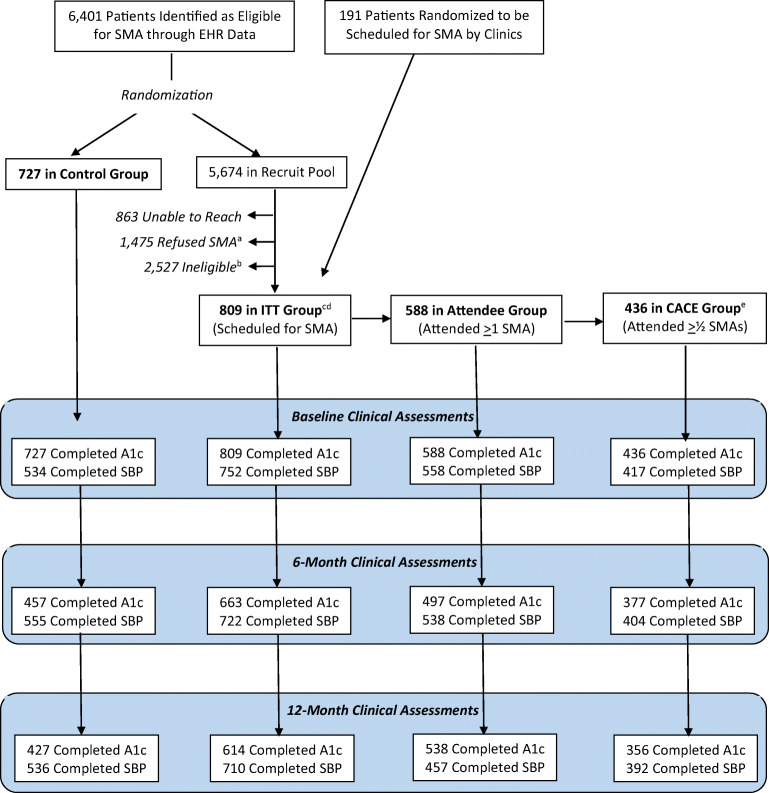
Research design and methods: A multi-site cluster randomized pragmatic trial examining implementation in clinical practice of diabetes SMAs in five Veterans Affairs (VA) health systems was conducted from 2016 to 2020 among 1537 adults with type 2 diabetes and elevated A1cs. Eligible patients were randomly assigned to either: (1) invitation to participate in a series of SMAs totaling 8-9 h; or (2) continuation of usual care. Relative change in A1c (primary outcome) and in systolic blood pressure, insulin starts, statin starts, and anti-hypertensive medication classes (secondary outcomes) were measured as part of usual clinical care at baseline, at 6 months and at 12 months (~7 months after conclusion of the final SMA in four of five sites). We examined outcomes in three samples of SMA participants: all those scheduled for a SMA, those attending at least one SMA, and those attending at least half of SMAs.
Results: Baseline mean A1c was 9.0%. Participants scheduled for an SMA achieved A1c reductions 0.35% points greater than the control group between baseline and 6-months follow up (p = .001). Those who attended at least one SMA achieved reductions 0.42 % points greater (p < .001), and those who attended at least half of scheduled SMAs achieved reductions 0.53 % points greater (p < .001) than the control group. At 12-month follow-up, the three SMA analysis samples achieved reductions from baseline ranging from 0.16 % points (p = 0.12) to 0.29 % points (p = .06) greater than the control group.
Conclusions: Diabetes SMAs as implemented in real-life diverse clinical practices improve glycemic control more than usual care immediately after the SMAs, but relative gains are not maintained. Our findings suggest the need for further study of whether a longer term SMA model or other follow-up strategies would sustain relative clinical improvements associated with this intervention.
Trial registration: ClinicalTrials.gov ID NCT02132676.
Keywords: shared medical appointment, peer support, disease management, implementation, diabetes mellitus, pragmatic clinical trial.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
References
-
- Ligthart S, wan Herpt TTW, Leening MJG, et al. Lifetime risk of developing impaired glucose metabolism and eventual progression from prediabetes to type 2 diabetes: a prospective cohort study. Lancet Diabetes Endocrinol. 2016;4(1):44-51. - PubMed
-
- Davies MJ, D’Alessio DA, Fradkin J, et al. Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) Diabetes Care. 2018;41(12):2669–2701. doi: 10.2337/dci18-0033. - DOI - PMC - PubMed
-
- Kirsh S, Watts S, Schaub K, et al. Training Manual, VA Shared Medical Appointments for Patients with Diabetes: Maximizing Patient & Provider Expertise to Strengthen Care Management. 2008. http://www.queri.research.va.gov/tools/diabetes/shared-med-appt.pdf. Accessed 1 August 2016.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
