

Quantitative Assessment of Viral Dispersion Associated with Respiratory Support Devices in a Simulated Critical Care Environment
- PMID: 33534659
- PMCID: PMC8314904
- DOI: 10.1164/rccm.202008-3070OC
Quantitative Assessment of Viral Dispersion Associated with Respiratory Support Devices in a Simulated Critical Care Environment
Abstract
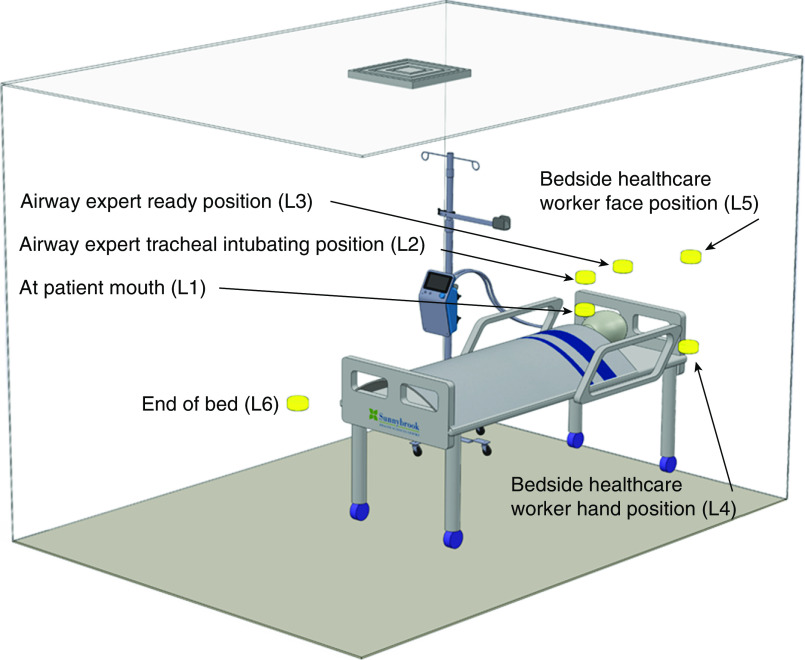
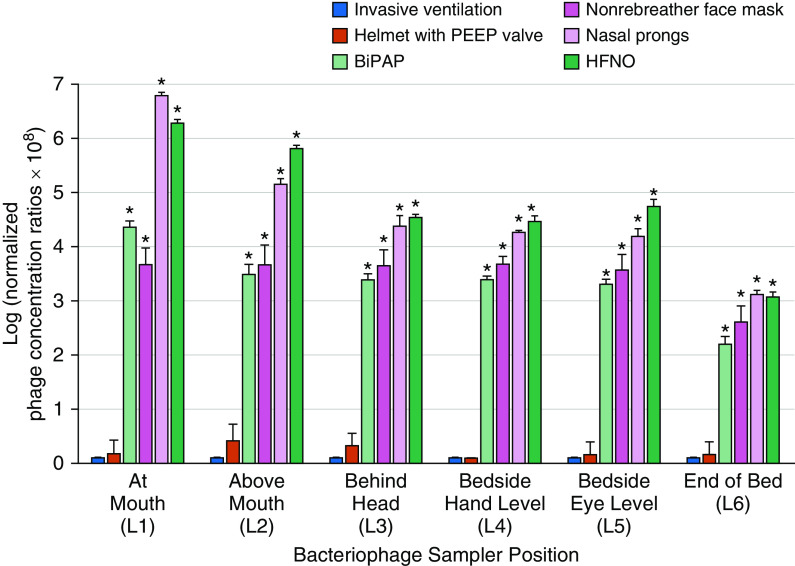
Rationale: Patients with severe coronavirus disease (COVID-19) require supplemental oxygen and ventilatory support. It is unclear whether some respiratory support devices may increase the dispersion of infectious bioaerosols and thereby place healthcare workers at increased risk of infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).Objectives: To quantitatively compare viral dispersion from invasive and noninvasive respiratory support modalities.Methods: This study used a simulated ICU room with a breathing-patient simulator exhaling nebulized bacteriophages from the lower respiratory tract with various respiratory support modalities: invasive ventilation (through an endotracheal tube with an inflated cuff connected to a mechanical ventilator), helmet ventilation with a positive end-expiratory pressure (PEEP) valve, noninvasive bilevel positive-pressure ventilation, nonrebreather face masks, high-flow nasal oxygen (HFNO), and nasal prongs.Measurements and Main Results: Invasive ventilation and helmet ventilation with a PEEP valve were associated with the lowest bacteriophage concentrations in the air, and HFNO and nasal prongs were associated with the highest concentrations. At the intubating position, bacteriophage concentrations associated with HFNO (2.66 × 104 plaque-forming units [PFU]/L of air sampled), nasal prongs (1.60 × 104 PFU/L of air sampled), nonrebreather face masks (7.87 × 102 PFU/L of air sampled), and bilevel positive airway pressure (1.91 × 102 PFU/L of air sampled) were significantly higher than those associated with invasive ventilation (P < 0.05 for each). The difference between bacteriophage concentrations associated with helmet ventilation with a PEEP valve (4.29 × 10-1 PFU/L of air sampled) and bacteriophage concentrations associated with invasive ventilation was not statistically significant.Conclusions: These findings highlight the potential differential risk of dispersing virus among respiratory support devices and the importance of appropriate infection prevention and control practices and personal protective equipment for healthcare workers when caring for patients with transmissible respiratory viral infections such as SARS-CoV-2.
Keywords: COVID-19; bacteriophage; bioaerosol; critical care; simulation.
Figures
Comment in
-
Mitigating Viral Dispersion during Respiratory Support Procedures in the ICU.Am J Respir Crit Care Med. 2021 May 1;203(9):1051-1053. doi: 10.1164/rccm.202102-0317ED. Am J Respir Crit Care Med. 2021. PMID: 33617748 Free PMC article. No abstract available.
-
Viral Dispersion in the ICU: The Wind Effect.Am J Respir Crit Care Med. 2021 Aug 15;204(4):488. doi: 10.1164/rccm.202105-1104LE. Am J Respir Crit Care Med. 2021. PMID: 34156905 Free PMC article. No abstract available.
-
Reply to Tandjaoui-Lambiotte et al.: Viral Dispersion in the ICU: The Wind Effect.Am J Respir Crit Care Med. 2021 Aug 15;204(4):489. doi: 10.1164/rccm.202105-1241LE. Am J Respir Crit Care Med. 2021. PMID: 34156912 Free PMC article. No abstract available.
References
-
- Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW, et al. the Northwell COVID-19 Research Consortium. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York city area. JAMA. 2020;323:2052–2059. [Published erratum appears in JAMA 323:2098.] - PMC - PubMed
-
- Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med. 2020;8:475–481. [Published erratum appears in Lancet Respir Med 8:e26.] - PMC - PubMed
-
- Grasselli G, Pesenti A, Cecconi M. Critical care utilization for the COVID-19 outbreak in Lombardy, Italy: early experience and forecast during an emergency response. JAMA. 2020;323:1545–1546. - PubMed
-
- Phua J, Weng L, Ling L, Egi M, Lim CM, Divatia JV, et al. Asian Critical Care Clinical Trials Group. Intensive care management of coronavirus disease 2019 (COVID-19): challenges and recommendations. Lancet Respir Med. 2020;8:506–517. [Published erratum appears in Lancet Respir Med 8:e42.] - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
