

Establishing Classifiers With Clinical Laboratory Indicators to Distinguish COVID-19 From Community-Acquired Pneumonia: Retrospective Cohort Study
- PMID: 33534722
- PMCID: PMC7901596
- DOI: 10.2196/23390
Establishing Classifiers With Clinical Laboratory Indicators to Distinguish COVID-19 From Community-Acquired Pneumonia: Retrospective Cohort Study
Abstract
Background: The initial symptoms of patients with COVID-19 are very much like those of patients with community-acquired pneumonia (CAP); it is difficult to distinguish COVID-19 from CAP with clinical symptoms and imaging examination.
Objective: The objective of our study was to construct an effective model for the early identification of COVID-19 that would also distinguish it from CAP.
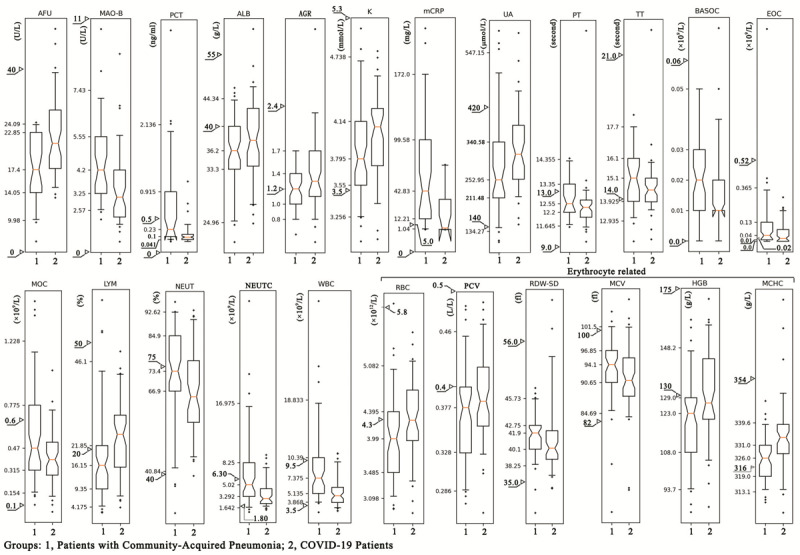
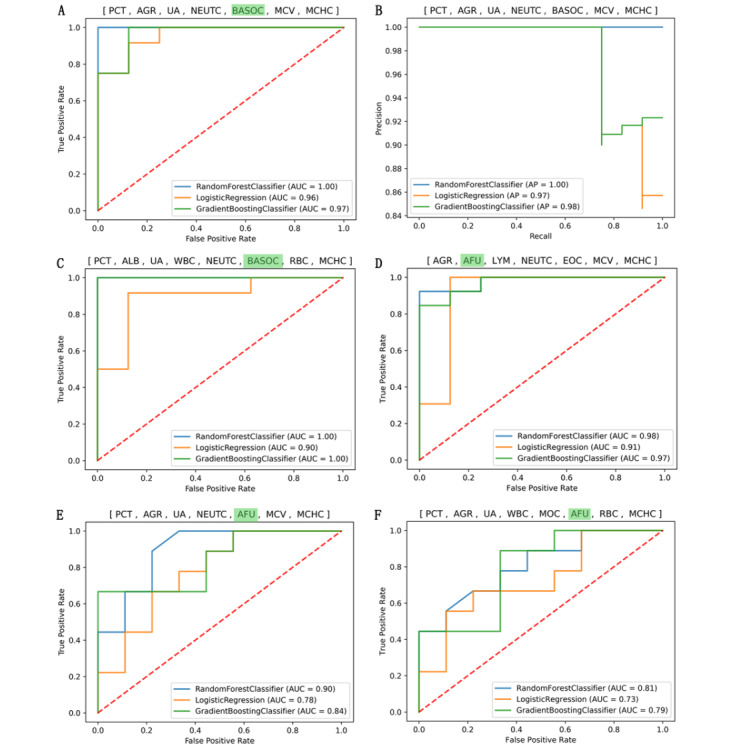
Methods: The clinical laboratory indicators (CLIs) of 61 COVID-19 patients and 60 CAP patients were analyzed retrospectively. Random combinations of various CLIs (ie, CLI combinations) were utilized to establish COVID-19 versus CAP classifiers with machine learning algorithms, including random forest classifier (RFC), logistic regression classifier, and gradient boosting classifier (GBC). The performance of the classifiers was assessed by calculating the area under the receiver operating characteristic curve (AUROC) and recall rate in COVID-19 prediction using the test data set.
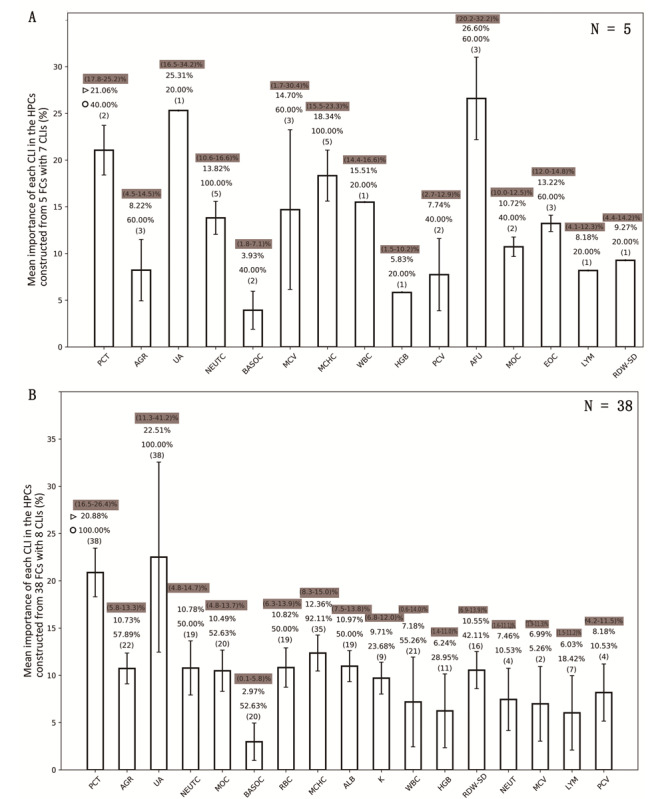
Results: The classifiers that were constructed with three algorithms from 43 CLI combinations showed high performance (recall rate >0.9 and AUROC >0.85) in COVID-19 prediction for the test data set. Among the high-performance classifiers, several CLIs showed a high usage rate; these included procalcitonin (PCT), mean corpuscular hemoglobin concentration (MCHC), uric acid, albumin, albumin to globulin ratio (AGR), neutrophil count, red blood cell (RBC) count, monocyte count, basophil count, and white blood cell (WBC) count. They also had high feature importance except for basophil count. The feature combination (FC) of PCT, AGR, uric acid, WBC count, neutrophil count, basophil count, RBC count, and MCHC was the representative one among the nine FCs used to construct the classifiers with an AUROC equal to 1.0 when using the RFC or GBC algorithms. Replacing any CLI in these FCs would lead to a significant reduction in the performance of the classifiers that were built with them.
Conclusions: The classifiers constructed with only a few specific CLIs could efficiently distinguish COVID-19 from CAP, which could help clinicians perform early isolation and centralized management of COVID-19 patients.
Keywords: COVID-19; classification algorithm; classifier; clinical laboratory indicators; community-acquired pneumonia.
©Wanfa Dai, Pei-Feng Ke, Zhen-Zhen Li, Qi-Zhen Zhuang, Wei Huang, Yi Wang, Yujuan Xiong, Xian-Zhang Huang. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 22.02.2021.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Coronavirus disease (COVID-19) pandemic. World Health Organization. 2020. [2020-05-06]. https://www.who.int/emergencies/diseases/novel-coronavirus-2019.
-
- Coronaviridae Study Group of the International Committee on Taxonomy of Viruses The species severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat Microbiol. 2020 Apr;5(4):536–544. doi: 10.1038/s41564-020-0695-z. http://europepmc.org/abstract/MED/32123347 - DOI - PMC - PubMed
-
- Ye F, Xu S, Rong Z, Xu R, Liu X, Deng P, Liu H, Xu X. Delivery of infection from asymptomatic carriers of COVID-19 in a familial cluster. Int J Infect Dis. 2020 May;94:133–138. doi: 10.1016/j.ijid.2020.03.042. https://linkinghub.elsevier.com/retrieve/pii/S1201-9712(20)30174-0 - DOI - PMC - PubMed
-
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020 Apr 07;323(13):1239–1242. doi: 10.1001/jama.2020.2648. - DOI - PubMed
-
- Zhang J, Tian S, Lou J, Chen Y. Familial cluster of COVID-19 infection from an asymptomatic. Crit Care. 2020 Mar 27;24(1):119. doi: 10.1186/s13054-020-2817-7. https://ccforum.biomedcentral.com/articles/10.1186/s13054-020-2817-7 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
