

Shaken Baby Syndrome: Magnetic Resonance Imaging Features in Abusive Head Trauma
- PMID: 33535601
- PMCID: PMC7912837
- DOI: 10.3390/brainsci11020179
Shaken Baby Syndrome: Magnetic Resonance Imaging Features in Abusive Head Trauma
Abstract
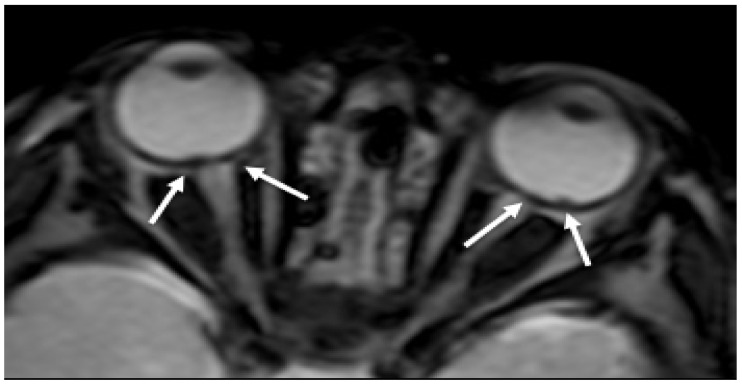
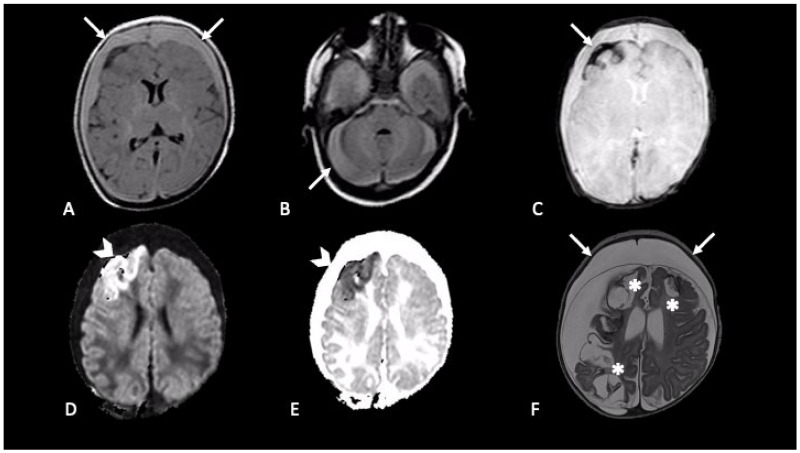
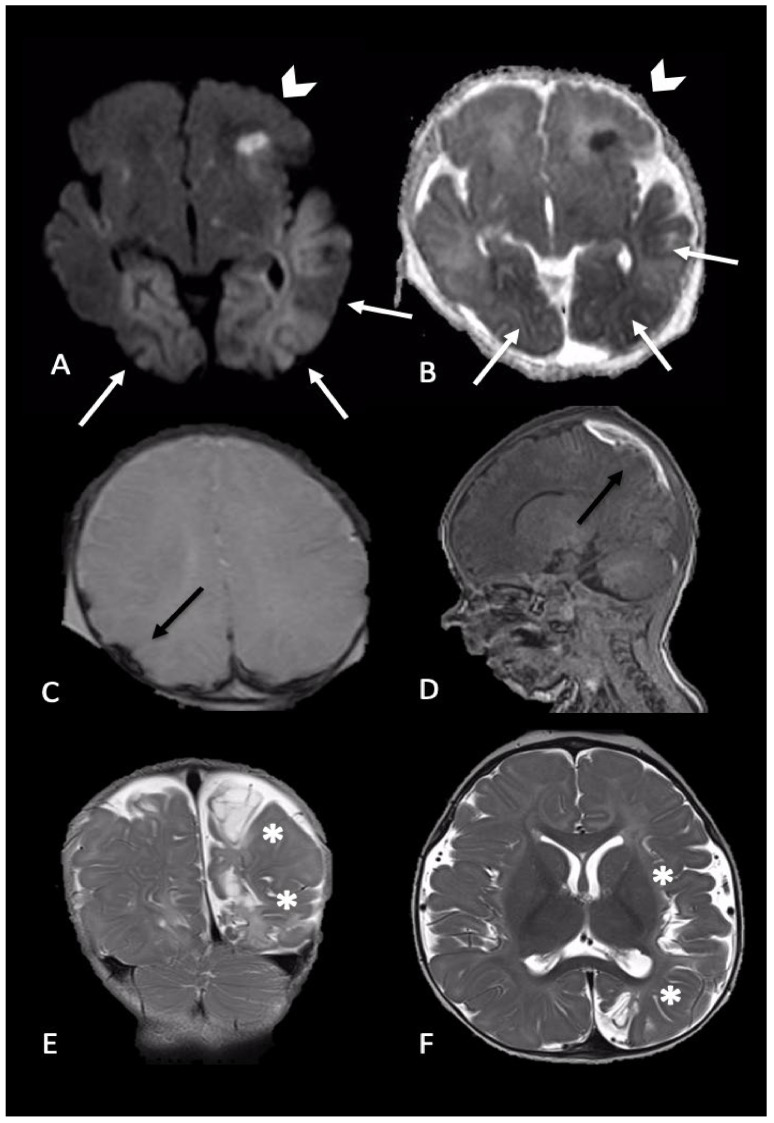
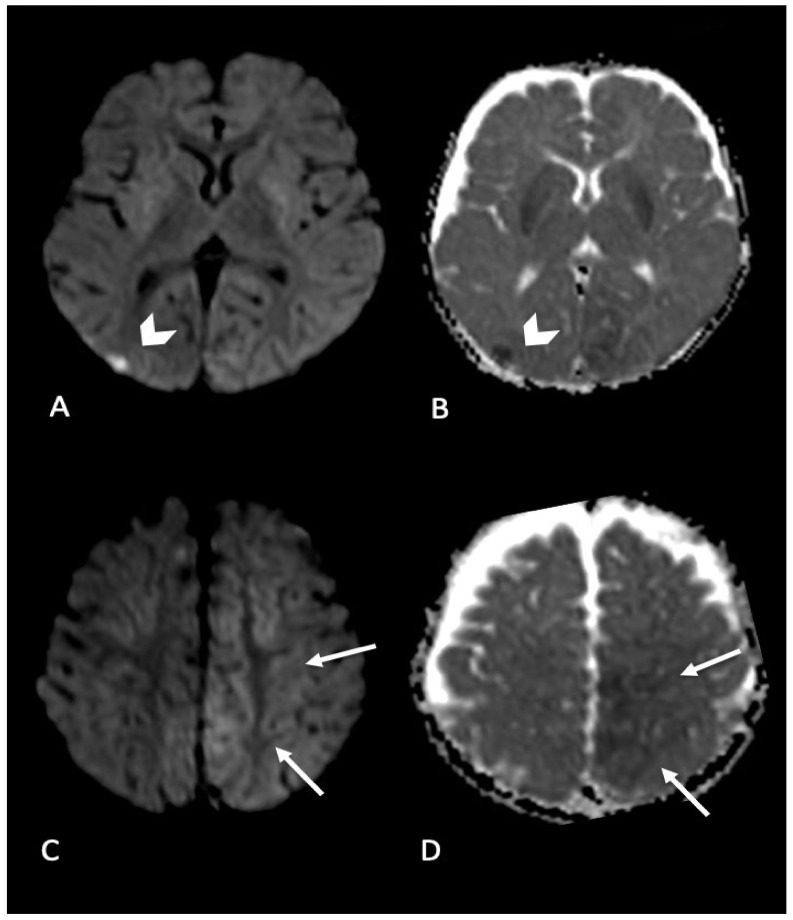
In the context of child abuse spectrum, abusive head trauma (AHT) represents the leading cause of fatal head injuries in children less than 2 years of age. Immature brain is characterized by high water content, partially myelinated neurons, and prominent subarachnoid space, thus being susceptible of devastating damage as consequence of acceleration-deceleration and rotational forces developed by violent shaking mechanism. Diagnosis of AHT is not straightforward and represents a medical, forensic, and social challenge, based on a multidisciplinary approach. Beside a detailed anamnesis, neuroimaging is essential to identify signs suggestive of AHT, often in absence of external detectable lesions. Magnetic resonance imaging (MRI) represents the radiation-free modality of choice to investigate the most typical findings in AHT, such as subdural hematoma, retinal hemorrhage, and hypoxic-ischemic damage and it also allows to detect more subtle signs as parenchymal lacerations, cranio-cervical junction, and spinal injuries. This paper is intended to review the main MRI findings of AHT in the central nervous system of infants, with a specific focus on both hemorrhagic and non-hemorrhagic injuries caused by the pathological mechanisms of shaking. Furthermore, this review provides a brief overview about the most appropriate and feasible MRI protocol to help neuroradiologists identifying AHT in clinical practice.
Keywords: MRI; abusive head trauma; child; infant; neuroimaging; shaking mechanism.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Parks S.E., Kegler S.R., Annest J.L., Mercy J.A. Characteristics of fatal abusive head trauma among children in the USA: 2003–2007: An application of the CDC operational case definition to national vital statistics data. Inj. Prev. 2012;18:193–199. doi: 10.1136/injuryprev-2011-040128. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
