

Diagnostic and severity scores for Cockayne syndrome
- PMID: 33536051
- PMCID: PMC7860636
- DOI: 10.1186/s13023-021-01686-8
Diagnostic and severity scores for Cockayne syndrome
Abstract
Background: Cockayne syndrome is a progressive multisystem genetic disorder linked to defective DNA repair and transcription. This rare condition encompasses a very wide spectrum of clinical severity levels ranging from severe prenatal onset to mild adult-onset subtypes. The rarity, complexity and variability of the disease make early diagnosis and severity assessment difficult. Based on similar approaches in other neurodegenerative disorders, we propose to validate diagnostic and severity scores for Cockayne syndrome.
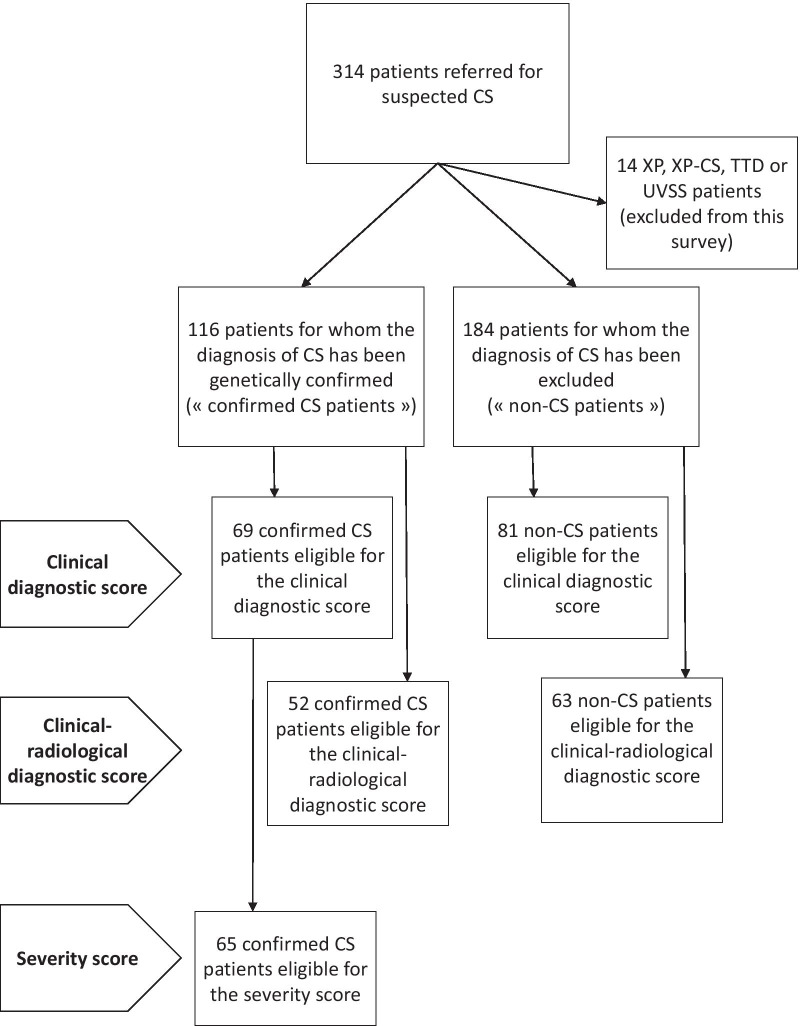
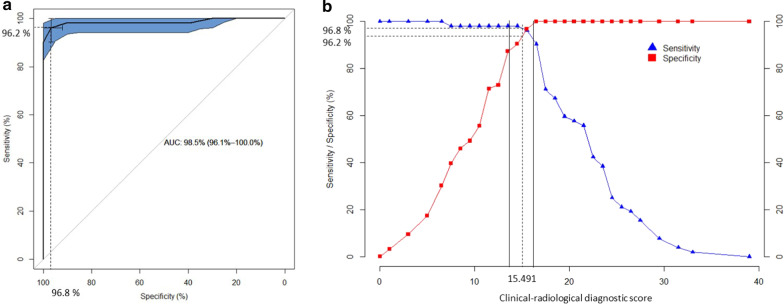
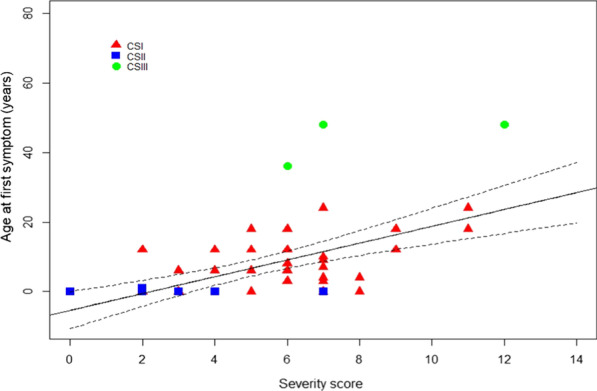
Methods: Clinical, imaging and genetic data were retrospectively collected from 69 molecularly confirmed CS patients. A clinical diagnostic score and a clinical-radiological diagnostic score for CS were built using a multivariable logistic regression model with a stepwise variable selection procedure. A severity score for CS was designed on five items (head circumference, growth failure, neurosensorial signs, motor autonomy, communication skills) and validated by comparison with classical predefined severity subtypes of CS.
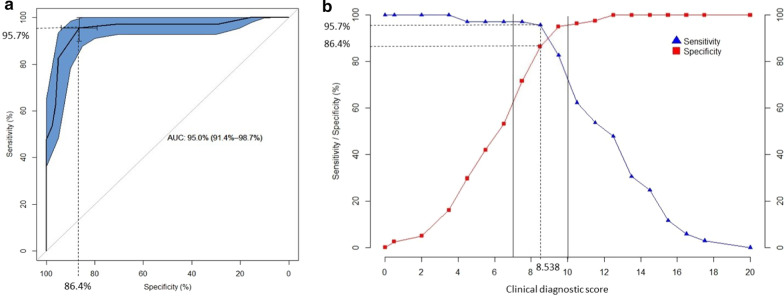
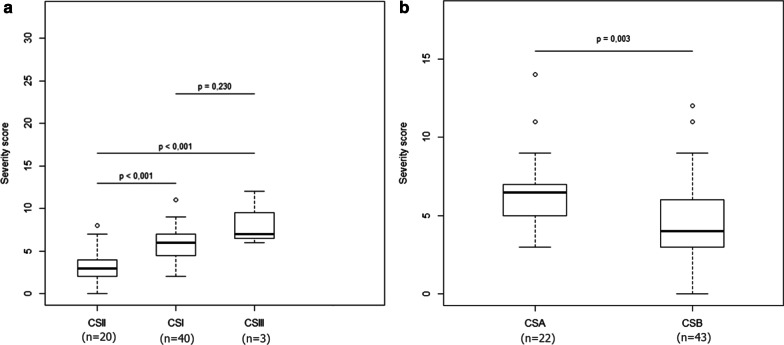
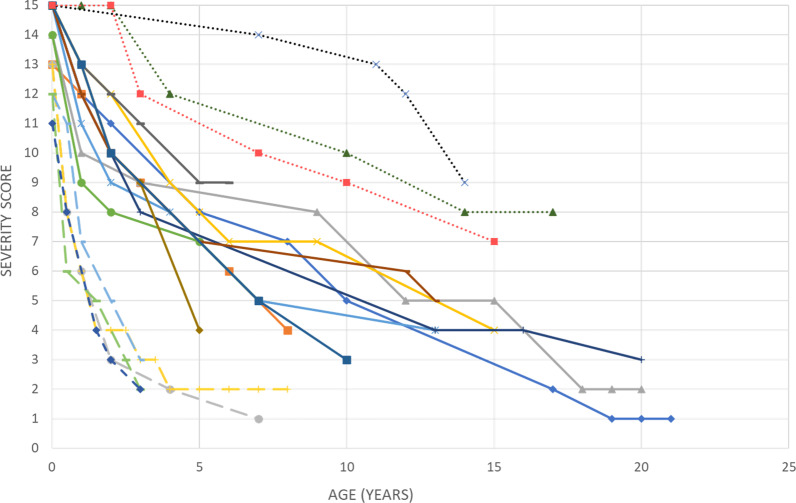
Results: Short stature, enophtalmos, hearing loss, cataracts, cutaneous photosensitivity, frequent dental caries, enamel hypoplasia, morphological abnormalities of the teeth, areflexia and spasticity were included in the clinical diagnostic score as being the most statistically relevant criteria. Appropriate weights and thresholds were assigned to obtain optimal sensitivity and specificity (95.7% and 86.4% respectively). The severity score was shown to be able to quantitatively differentiate classical predefined subtypes of CS and confirmed the continuous distribution of the clinical presentations in CS. Longitudinal follow-up of the severity score was able to reflect the natural course of the disease.
Conclusion: The diagnostic and severity scores for CS will facilitate early diagnosis and longitudinal evaluation of future therapeutic interventions. Prospective studies will be needed to confirm these findings.
Keywords: Clinical severity; Cockayne syndrome; Diagnosis; Score.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Mayne LV, Lehmann AR. Failure of RNA synthesis to recover after UV irradiation: an early defect in cells from individuals with Cockayne's syndrome and xeroderma pigmentosum. Cancer Res. 1982;42(4):1473–1478. - PubMed
-
- Lehmann AR, Kirk-Bell S, Mayne L. Abnormal kinetics of DNA synthesis in ultraviolet light-irradiated cells from patients with Cockayne's syndrome. Cancer Res. 1979;39(10):4237–4241. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
